Biography
Interests
Anas Ahmad Aladnani1* & Mohammed Al Sobeai2
1Orthopaedic Surgery, King Fahad Armed Forces Hospital, Jeddah, Saudi Arabia
2Department of Orthopedic Surgery, Dr. Soliman Fakeeh Hospital, Jeddah, Saudi Arabia
*Correspondence to: Dr. Anas Ahmad Aladnani, Orthopaedic Surgery, King Fahad Armed Forces Hospital, Jeddah, Saudi Arabia.
Copyright © 2019 Dr. Anas Ahmad Aladnani, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Gout is one of the types of inflammatory arthritis that can affect anyone. It is commonly seen in Orthopedic practice and usually included in the differential diagnosis of mono- or polyarthralgia. Occasionally, the disease is associated with swelling and/or lesion affecting lower limb joints more than other joints in the body. In this case report we present an atypical presentation of gout in a middle aged man presented with relatively large tumor-like lesion in the ankle joint. The treatment of gout is focused on medical more than surgical treatment . Surgery is reserved for large Lesions or Lesions that involve important joints like weight bearing joints to prevent permanent damage and potential disability.
Introduction
Gout is a common cause for joint disease affecting men more than women with an average from 40-
60 years of age. It’s caused by a defect of Purine nucleic acid metabolism leading to Hyperuricemia. The
pathophysiology of the disease involves deposition of Monosodium urate crystals which in turn trigger an
inflammatory reaction including activation of platelets, complement system and IL-1 production. Patients
usually present with recurrent attacks of lower limb joint pain most commonly in the big toe “podagra”. Less
common sites include ear helix, eyelid, olecranon, Achilles’ tendon and spine. Radiographic signs may show punched out periarticular erosions with sclerotic overhanging borders. Also, may show soft tissue lesion
known as “Tophi” [1]. Correctly diagnosing gout and differentiating it from other inflammatory arthritic
conditions, such as rheumatoid arthritis, septic arthritis, and inflammatory episodes of osteoarthritis, is
important, because treatment of these conditions differ [2]. Nevertheless, the gold standard diagnostic tool in
diagnosing gout is joint aspiration and crystal analysis which reveals thin, tapered, needle-shape intracellular
crystals and strongly negative birefringent. The management of gout often relies on medical therapy and
diet modification. However, surgery may be indicated in some patients with severe joint destruction or
superinfection. Less frequently, patients may present with largely destructive Tophi around the joints. In
such cases, surgical resection is indicated to prevent joint damage [3]. Here, we present a case report for a
patient presented with large tophaceous lesion involving the Right ankle and foot and another small lesion
in the Left little toe.
Case
A 53 year-old male with a long history of gout “ not compliant to medication” presented to orthopedic clinic
with multiple masses in different sizes and locations . His main problem is inability to put foot wear due to
large mass on Right ankle and painful left little toe. Patient gave history of previous surgical debridement
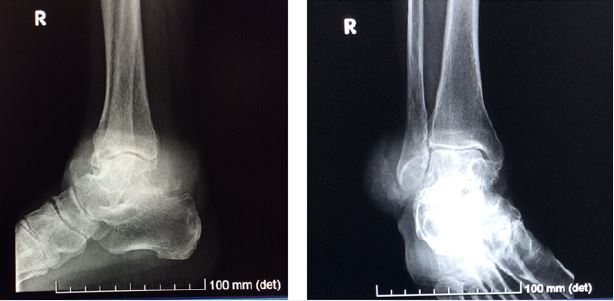
for the left little toe mass 4 years prior to presentation. On Examination, the ankle mass was large measuring
8*8cm over the lateral malleolus with overlying skin discoloration that is almost erupted. Also, Multiple
small masses on the dorsal and lateral aspects of the foot were identified (Figure 1). The left little toe mass
was relatively small measuring 3*3cm involving most of the dorsal aspect of the toe.


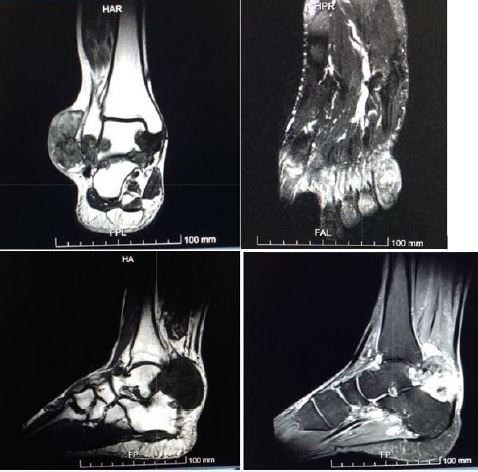
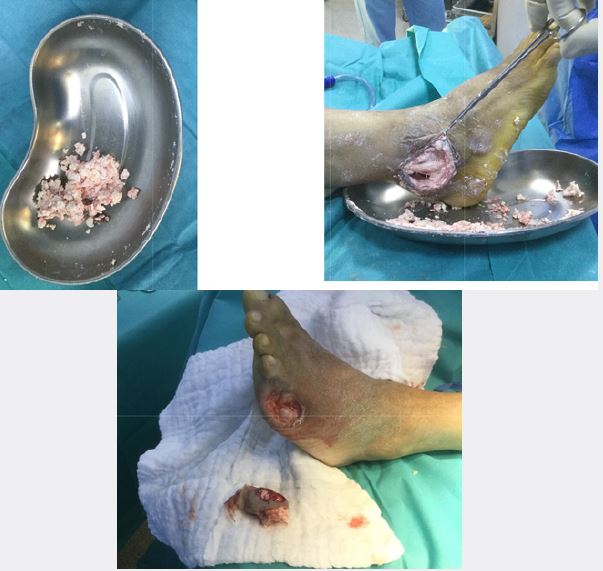
MRI of right ankle showed heterogeneous soft tissue mass measuring 6*2.2*5cm involving the lateral ankle and another mass measuring 8*4.3*4.7cm at the posterior aspect of the ankle encasing lateral and medial tendon groups. Anterior ankle and subtalar joints are preserved (Figure 4). The patient was prepared for surgical intervention to relieve his pain and reduce the size of the lesion to help him use regular foot wear. Debulking of the right ankle lesion was done as well as amputation of the left little toe as the bone was completely destroyed and the mass was fungating.
Intraoperatively, the ankle mass contains white small multiple hard fragmented substances (Figure 5). Specimens were sent for histopathology. Wound irrigated and closed primary. In the immediate post operative period, patient was in a good medical condition, below knee splint was applied and the patient was instructed for protected weight bearing (PWB) using crutches. We followed up the patient in the clinic as regular visits, sutures were removed after 2 weeks and the wounds were healed without complications. Histopathology result of the lesion was consistent with Tophaceous gout. One week after, we started weaning the patient from crutches and allowed full weight bearing (FWB). Patient was followed up by rheumatologist simultaneously.
Discussion
Thorough review of articles which discussed the surgical intervention of Tophaceous gouty lesions in the
foot and ankle showed that surgical treatment is an advantage in a way that it prevents complications and
disability [4]. There is a limited literature on the surgical treatment of tophaceous gout. No study has been
published with statistically robust data on specific outcome measures. The lack of controlled clinical studies
makes it a challenge to determine when, or if, a specific patient should be referred for surgery to remove
tophi. In addition, there is no clear consensus regarding how to define “refractory gout,” how common it is,
and how long medical therapy should be administered before resorting to surgery.
In rare cases, amputation may be the only viable option. Amputation is typically reserved for the hypovascular foot arising either from peripheral vascular disease or severe vascular impairment following extensive debridement of tophi. In addition, amputation may be the best option when patients have a non reconstructible deformity secondary to extensive bone destruction or bone loss from surgical resection and/or debridement [5]. In their case report, Kerim et al concluded that early surgical treatment may prevent extremity loss and further complications. In severe cases especially with compliance issues, amputation provides acceptable results [3].
Conclusion
Tophaceous soft tissue lesions can present in large joints like the ankle and in relatively large sizes. Gouty
tophi should be the first differential diagnosis among soft tissue masses in gout patient. Early surgical
intervention maybe of great importance in order to prevent further permanent joint destruction and disability.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!