Biography
Interests
Buse Sener, P.T. & Feyza Sule Badilli Demirbas*, P.T., PhD.
Department of Physiotherapy and Rehabilitation, Faculty of Health Sciences, Yeditepe University, Istanbul, Turkey
*Correspondence to: Dr. Feyza Sule Badilli Demirbas, Department of Physiotherapy and Rehabilitation, Faculty of Health Sciences, Yeditepe University, Istanbul, Turkey.
Copyright © 2019 Dr. Feyza Sule Badilli Demirbas, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Comparative, repeated-measures study
To examine the immediate effect of abdominal drawing-in maneuver (ADIM) using a pressure
biofeedback unit (PBU) on electromyography (EMG) signal amplitude of the hip abductor, knee
external rotator and ankle inverter during resisted strengthening exercises in supine position.
The ADIM is used to prevent abnormal movements of the pelvis during exercises. Performing an
ADIM may increase the activities of hip abductor, knee external rotator and ankle inverter muscles which are weak in individuals with anterior pelvic tilt. These exercises with ADIM may decrease
the angle of pelvic tilt.
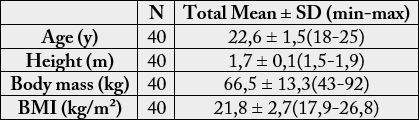
Forty individuals (20 men, 20 women) with anterior pelvic tilt, aged 18 to 25 years (mean±SD,
22,6±1,5 years) were recruited for this study. Transverse abdominis muscle contraction with ADIM
was examined by a pressure biofeedback unit. Resisted strengthening exercises with Thera-Band
have been performed for hip abduction, knee external rotation and ankle inversion in supine position.
The EMG signal amplitudes were measured during exercises with and without ADIM. Surface
EMG signals were recorded from gluteus medius, biceps femoris and tibialis anterior muscles.
There were significant differences in the activations of muscles with and without ADIM. The
EMG amplitude increased during ADIM in the gluteus medius (mean±SD, 59±21 versus 85±31;
P<,001), biceps femoris (mean±SD, 29±15 versus 40±18; P<,001) and tibialis anterior (mean±SD,
48±20 versus 67±25; P<,001).
Based on these findings, gluteus medius, biceps femoris and tibialis anterior is activated by using
ADIM. Therefore, ADIM could be used as an effective method to correlate the muscles activation
during exercises in the individuals with anterior pelvic tilt.
Introduction
Stabilization exercise is an effective intervention method for relieving the pain and dysfunction associated
with low back pain [1]. Stabilization exercises based on the abdominal drawing-in maneuver are widely used
to contract the TrA [2]. This method retrains the deep muscles using isometric contractions [3], minimal
contractions of the large muscles, and selective contraction of the TrA [4].
The abdominal drawing-in maneuver (ADIM) is a lumbar stabilization exercise that is mainly performed [5- 7]. The ADIM re-educates TrA and is therefore effective at relieving dysfunction [8]. ADIM can effectively improve the lumbo-pelvic stabilization in adults with core instability [9].
The abductor muscles have important kinesiologic roles in standing on feet and ambulation in humans [10]. The gluteus medius muscle controls movements of the femur and stabilizes the pelvis during mobilization of the lower extremities. Strengthening exercises for gluteus medius muscle were shown to improve movement in the lower extremities, prevent injuries, and reduce pain [11].
The internal femur rotation can influence sagittal pelvis motion. On average, for every 5º of anterior pelvis tilt there was 1.2-1.6º of internal femur rotation and the converse was true for posterior pelvis tilt and external femur rotation. Altered pelvis movement in the sagittal plane may influence transverse femur motion [12].
Internal tibial rotation is increased or prolonged with excessive pronation of the subtalar joint (STJ). It describes the effect of excessive STJ pronation on the tibiofemoral joint, the possible compensatory action of the femur to deal with the excessive pronation, and the resulting path-mechanics at the patellofemoral joint [13].
The position of hip is associated with subtalar joint. During weight-bearing, medially rotating the hip results in subtalar joint supination, while laterally rotating the hip results in subtalar joint pronation [14,15].
A combined effect of rotational alignment between segments and the cumulative effect of foot hyper pronation on pelvic tilt revealed that only the shank significantly affected pelvic alignment, acting as a mediator between a foot and a thigh with the thigh having a crude significant effect on the pelvis. When internal rotation of the shank occurs, calcaneal eversion couples with thigh internal rotation and anterior pelvic tilt. It can be concluded that in response to induced hyper pronation, the shank is a pivotal segment in postural adjustment [16].
The importance of this study is to demonstrate the additive effect of ankle dorsiflexion on deep core muscle thickness and activity, thus contributing to existing knowledge about therapeutic exercise for the effective management of low back pain [17].
Methods
The subjects of the present study were 21 healthy males and 22 healthy females with anterior pelvic tilt
who were explained the purpose and method of the study, and who voluntarily agreed to participate in the
study. Subjects who had neurological, musculoskeletal or cardiopulmonary disease or who had contracture
at the hip, knee or ankle were excluded. Three participants (1 males, 2 female) could not effectively perform
ADIM and were excluded from the analysis of the present study. Therefore, the final study subjects were 40
persons (20 males, 20 females) and their mean age, height, weight and BMI were 22.6±1.5 years, 1.7±0.1m,
66.5±13.3kg, and 21.8±2.7kg/m2, respectively (Table-1). All subjects signed an informed consent and this
study was approved by Yeditepe University Clinical Research Ethics Committee.
The inclinometer technique was adopted for measuring the flexion range of motion (ROM) of the lumbar spine [18]. The inclinometer with the two-point contact at its base was used BASELINE Gravity Inclinometer. It was positioned in the L5-S1 landmark to measure the anterior pelvic tilt movement. The participants were asked first to stand in their usual, relaxed posture [19]. Normal pelvic angle ranges are between 7º and 15º. Abnormal pelvic tilt or anterior pelvic tilt was recorded as present when the ASIS level was lower than the PSIS with more than 15º tilt [20]. Individuals who have more than 15º tilt were selected.
PBUs are used for clinical evaluation of the abdominal muscles, but it can also provide feedback to subjects who are receiving motor control training [21]. In the case of ADIM, the prone and supine positions can be employed when using a PBU [22]. In the supine position, the PBU is placed below the lumbar lordosis and air is infused into the bulb to create a pressure of 40mmHg [23]. For successful ADIM, rather than using large PBU pressure increases, exercises that promote slight increases of around 0-2mmHg from a baseline of 40mmHg are desirable [24]. Individuals were asked to perform hip abduction, knee external rotation and ankle inversion exercises. ADIM was taught and then exercises were repeated.

EMG data were collected using a Chattanooga Intellect Advanced Color Combo + EMG. The electrode sites were shaved and cleaned with rubbing alcohol to prepare the skin. Double electrodes for each muscle were positioned at a fixed interelectrode distance of 1-3cm. EMG data were collected for the following muscles of the dominant lower extremity: gluteus medius (in the middle of the muscle, on an oblique angle at, or slightly above, the level of the trochanter), biceps femoris (parallel to the muscle fibers, on the lateral and posterior aspect of the thigh, approximately half the distance between the gluteal fold and the popliteal fold) and tibialis anterior (parallel to the muscle fibers, on the lateral and anterior aspect of the lower leg, closer to the knee between the knee fold and ankle fold). The 3 trials of 10-second voluntary contraction were calculated for each muscle. the EMG signal was collected, the data for each trial were expressed and the average of 3 trials was used for analysis.
Data were entered into a database and analyzed using IBM SPSS version 22. Descriptive statistics were calculated for demographic information. General characteristics of the subjects and all variables were computed and expressed as means ± standard deviations. A One-sample t-test was used to compare the muscle activations of the hip abductor, knee external rotator and ankle inverter to verify differences for exercises with and without ADIM. A p value of ≤0.05 was considered statistically significant.
Results
There is a difference in the scores for the muscle activations of muscles with ADIM and without ADIM. The
scores for the activations without ADIM is lesser than the scores for the activations with ADIM (Table-2).
One-sample T-test was conducted to compare the differences between activations without ADIM and the activations with ADIM.
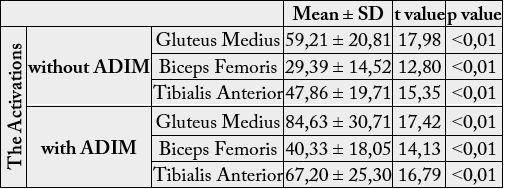
EMG measures were analyzed with One Sample T-Test (Figure-1). The correlation of the activations of muscles with and without ADIM were shown below.
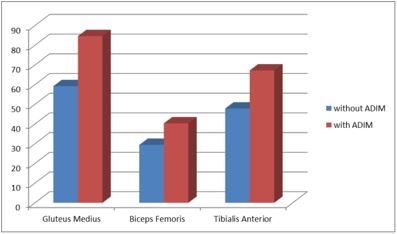
There were statistically significant differences in the scores. All correlations have obtained p<0.05 in %95 confidence interval.
Discussion
There are few studies in the literature showing the effects of the ADIM on the gluteus maximus, hamstrings,
erector spine and abdominal muscles during exercises. However, no study had investigated the effects of
performing an ADIM with a pressure biofeedback unit on the gluteus medius, biceps femoris and tibialis
anterior muscle activity during exercises. Like previous study [25], the effects of performing the ADIM
using a pressure biofeedback unit during prone knee flexion on the hamstrings and erector spine muscle
activity and on the amounts of pelvic motions and knee flexion. The findings suggest that the ADIM using
a pressure biofeedback decreased the activity of both erector spine muscles and increased the medial and
lateral hamstrings muscle activity. The amounts of anterior pelvic tilt, pelvic rotation, knee flexion, and
perceived pain also decreased more significantly in prone knee flexion with the ADIM than in the same
maneuver without the ADIM. Another previous study [26], showed that when performing an ADIM
during hip extension exercises done in a prone position, the EMO signal amplitude decreased significantly
in the erector spine and increased significantly in both the gluteus maximus and medial hamstrings. The
angle of anterior pelvic tilt decreased significantly during prone hip extension with an ADIM.
Surface EMG is a non-invasive method, but it is limited in its ability to detect fine activities of the located muscles. Fine-wire EMG can be used to observe these fine activities, but this is an invasive method and can cause pain and inflammation. According to Andrew [27], the global pattern of muscle recruitment was consistent between s EMG and f EMG, but s EMG recordings were characterized by additional myoelectric content. These findings support and guide the use of f EMG techniques to investigate leg muscle recruitment during cycling.
The clinical use of pressure biofeedback for assessing transverse abdominis (TrA) activation during a supine ADIM. Identification of an inability to maintain pressure during an ADIM may be of limited clinical value, but the ability to maintain pressure provides no information regarding TrA activation. According to Dustin, clinicians and researchers who rely on pressure biofeedback to assess TrA function during an ADIM performed in supine [18].
The study had several limitations. First, we examined the immediate effects of ADIM for the muscle activations. Therefore, further studies are needed to investigate the long-term effects of ADIM performance on the muscle activations. Secondly, an ADIM performed in supine is associated with pressure biofeedback as an assessment tool for local muscle function.
Conclusion
This study aimed to investigate the changes in the muscle activations of the gluteus medius, biceps femoris
and tibialis anterior after ADIM performance during hip abduction, knee external rotation and ankle
inversion in 40 subjects, and to verify the effects of ADIM on anterior pelvic tilt to determine its clinical
usefulness.
The results of this study showed significant differences at gluteus medius, biceps femoris and tibialis anterior muscle activations with ADIM. Therefore, the results of this study support the hypothesis that the ADIM performance in anterior pelvic tilt would affect the activations of the weak muscle groups. The resisted strengthening exercises for hip abduction, knee external rotation and ankle inversion should be included in the exercise program for the individual with anterior pelvic tilt.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!