Biography
Interests
Elizabeta Popova Ramova1* & Leonid Ramov2
1Training Implementation Center Bitola, R. Macedonia
2Medical Middle School. St. Luka, Skopje
*Correspondence to: Dr. Elizabeta Popova Ramova, Training Implementation Center Bitola, R. Macedonia.
Copyright © 2019 Dr. Elizabeta Popova Ramova, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Leg treads are common in people who are bruised professionally, such as athletes and professional soldiers and police officers. In our case, we have an overview of the treatment of the ankle in a high school student, injured at the class of physical education. The goal of our research is to present the protocol for rehabilitation in acute and subacute conditions with the effects of treatment in ankle sprain injury.
The injury occurred at a 16 year old boy, for the second time during physical education class. After
the x-ray picture image and examination by an orthopedist, bone injury was excluded, he was sent
home with analgesics, unloading and resting. Physical procedures were included on the second day
after the injury in the following order: polarized light 20min. Low energy laser for 15 minutes, cryo
massage, lymphatic drainage and typing. The effect of the treatment was evaluated through the size
of swelling, movement range and pain assessment.
In 10 days of treatment, with partially present pain at the load, the student returned to teaching,
with a break from physical education for another 2 weeks.
Modern physical modalities and apparatus techniques are in constant development in physical
medicine. Luminous therapy has good results in withdrawal of swelling and anesthesia. Modern
treatments like LLLT and Typing are in our healthcare system borne by the patient and can not be
made available to any patient.
The application of multiple physical modalities along with the type provides good results in terms
of improving mobility and pain relief in patients with a ankle sprain, which goes with a quick return
to work tasks, and shortening the time for sick leave.
Introduction
Injuries to the ankle are one of the most frequent in the presence of the emergency intervention unit, and
they are frequent among high school students either to take care or not to play sports [1]. In our previous
work experience, we had a large number of patients who came for rehabilitation after ankle sprain injury
at work such as police officers, soldiers and officers. They arrive for rehabilitation after surgical conservative
treatment with gypsum immobilization from 14-21 days. Beginning of rehabilitation after 14, or 21 days,
prolongs the time of absence from work. Such injuries can be a cause of poor quality of life later due to
leg pain in the professional eligibility [2]. The every guideline for ankle sprain treatment must have the
diagnosis, prevention and therapeutic interventions for ankle sprains by updating the existing guideline
and incorporate new research [3]. A secondary objective was to provide an update related to the costeffectiveness
of diagnostic procedures, therapeutic interventions and prevention strategies. Early involvement
of rehabilitation is possible if instead of gypsum immobilization a solid orthoses of the ankle is given,
and involve physical modalities with anti-oedematous and analgesic action. Ankle sprains, are a common
problem in sports and medical care. Ankle sprains result in pain and absenteeism from work and/or sports
participation, and can lead to physical restrictions such as ankle instability. Nowadays, treatment of ankle
injury basically consists of immobilization, ice, and out of weight [4]. The these physical modalities, such
as polarized light, low energy laser, lymphatic drainage, and functional typing, are not paid by the patient’s
health insurance, so they are not available to every patient. Early included treatment, rehabilitation, and
secondary prevention of ankle injuries can limit the amount of time absenteeism from physical activity and
work and avoid negative long-term sequels [5].
The purpose of our research is to present the protocol for rehabilitation in acute and sub acute conditions with the effects of treatment in ankle sprain injury.
Material and Method
In our case report research we have represent a case of ankle sprain treatment of right leg, by 16 years old
middle school boy. He was transported to emergency unit with out of weight of his leg, and have been
examination from orthopedic surgery doctor. The x-ray picture excluded bone trauma. He was treated with
immobilization with bandage and sent home with out of weight and medical support of analgesic and
enzymes pills. The same day the leg was in position of elevation and with application of ice in ankle sprain
region of foot.
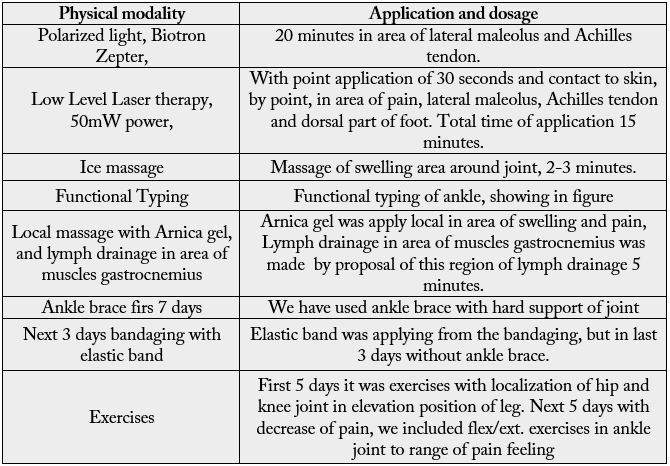
With rehabilitation was started next day, and it is use in follow 10 days with follow program step by step showing in table 1.
The evaluation of treatment was made with three scores before and after 10 days of treatment, and differences of proportion with T-test, and significances p,0.05.
1. Size of swelling
2. Range of motion in ankle flexion/extension,
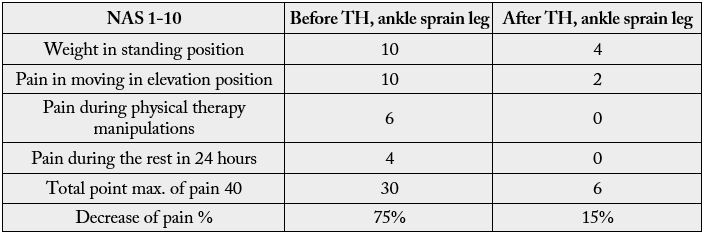
3. Assessment of pain with NAS, scale








Results
The results from scores are showing in table 2 ,3 and 4.


The total effect of rehabilitation is made with one point for every percentage of goodness before and after treatment. It is showing in table 5.
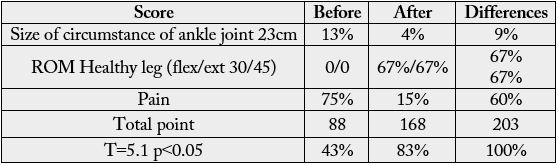
Statistical evaluation with differences of proportion showing significant goodness of condition before and after treatment T=5.1, p<0.05
Discussion
Ankle sprain is the most common injury in professional sport men, but also in athletics in schools according
22.6% of all injuries [6,7]. The high prevalence of ankle injuries in basketball can largely be attributed to the
nature of the sport, which involves rapid changes in direction, player contact, repetitive jumping, and landing
activities [8]. Our patient wanted the injury playing basketball at the time of physical education. It was his
second time with same injury.
Screening techniques are part of protocol after rehabilitation and pain relief to identifying at-risk athletes. Factors described in the literature that identify athletes at risk for ankle injuries include proprioceptive defects, weak postural sway scores, and a history of ankle sprains [9,10]. Our patient has a history of ankle sprain and shorter tractus iliotibialis muscles and flat food. Our school standard, do not need for physical education sport shoes with high quality, because the population cannot buy it. There are some standard protocols to accesss condition before and after treatment one of them is: Clinical assessment of acute lateral ankle sprain injuries (ROAST) [11]. It is consisting: numeric rating scale for pain, ankle joint swelling, ankle joint range of motion, weight bearing test, static postural balance impairment and visual assessment for antalgic gait. We have accessed our patient with three of them.
Early return to sport may increase risk for recurrence or chronic injuries. The time for ligament healing is 6-3 months, by some studies, and patients may have mechanical laxity up to a year after the injury. Early return to sport and interruption of rehabilitation programs after an ankle injury have been reported as problems in many sports [12,13]. Main cost for ankle sprain treatment is hospital care, rehabilitation/nursing care, and physical therapy [14].
Physical medicine applies physical modalities and assistive technology in rehabilitation process. We have used the modern treatment, and pay it by own, because it was our member of family, and we are experts in this part of rehabilitation. There are conflicting opinions about the effect of therapy in the acute stage of the injury [15,16]. We have our own experiences in the treatment of cold and interfering currents in the treatment of injuries [17,18].
We have analyzed the effect of them before and published in our research studies. In the second part or in chronic rehabilitation program, we apply exercises for balance and proprioception and elongation of short muscles groups. Ankle braces and other supports like bandaging and taping, are focused on swelling reduction and pain less with immobilization. They have effect to considered the injury and reduce time for returning to sports or other high-risk activities, and that was and our aim [19].
Light therapy is giving good results in swelling reduction and pain relief, but it is also very effective in ligament recovery [20]. There is no evident studies exactly for ankle sprain recovery, but we have our own long time experience [18].
Surgical treatment plays only a minor role for the treatment of acute ankle sprains only in the diagnostic process, or applying gypsum immobilization. In most narrative review articles non-operative treatment is recommended [21]. Program of treatment depends of health care program and payment of the health system in many low and middle economy countries.
We have used pain killer medicaments in first three days after injury, but physical medicine modalities are useful in non pharmacological treatment of pain and sweeling. Physical medicine doctors perform therapeutic interventions, such as stretching, manual therapy, electrotherapy, ultrasound, and exercises, to increase ankle mobility and decrease swelling and pain [22]. We have our own medical strategy to use everything who can decrease them with ice massage, light therapy, sonophoresis and electrical current, but in this case we have used only the therapy presented by our protocol for treatment [23-25].
Conclusion
Rehabissssslitation of patient after ankle sprain in acute and sub acute stages, depends of joint instability and
lesion of soft tissues. The role of therapy in those stages is to reduce swelling and pain, and support ligament
healing. Modern physical modalities like light therapy and functional type with out of weight of leg in first
7 days can short time of immobilization and prepare patient to came back to his work activity but it cannot
be a program for professional sport men. Sport men need in chronic stage more individual program.
Conflicts of Interests
Authors confirm that article have no conflict of interest.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!