Biography
Interests
Dr. Mohan Kumar, J.*, Dr. Vijay, M. & Dr. Mahesh, M. N.
Department of Orthopaedics, Sathya Sai Orthopaedic Hospital Bengaluru, India
*Correspondence to: Dr. Mohan Kumar, J., Department of Orthopaedics, Sathya Sai Orthopaedic Hospital, Bhattarahalli, Near RTO, KR Puram, Bengaluru - 560049, India
Copyright © 2018 Dr. Mohan Kumar, J., et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Management of fracture distal end clavicle is a controversial topic for orthopaedic surgeons. With a relatively active lifestyle, now a days patients want better results both cosmetically and functionally. There is no consensus regarding the gold standard treatment for this fracture, despite so much literature available for the management of this common fracture. We present here a technique of fracture stabilization using the metal button in a patient with a widely displaced Neer type IIB distal clavicle fracture. We have fixed the fracture by indirect technique, by using a metal button over the clavicle and Ethibond No 5 around the coracoid. The patient achieved satisfactory results after surgery; this technique is simple, reproducible and avoids the complications associated with implants and also cost effective.
Introduction
Distal clavicle fractures account for 10 to 15 % of all clavicle fractures [1-2]. These fractures have been classified by Neer into three types, with type IIB being difficult to treat due to displacement of the proximal fragment [2]. Though fracture of the shaft is the commonest, distal clavicle fractures constitutes 21-28% of all clavicle fractures. 10-52% of these distal clavicle are displaced fractures. Conservative treatment leads to high rate of non-union, hence surgical treatment is ideal [3-5]. It has been shown that if conoid ligament disruption is left untreated, the risk of non-union increases, so to avoid superior migration of the proximal fragment, surgical strategies should include reconstruction of the disrupted conoid ligament [6]. A wide variety of operative techniques have been described to treat these injuries, the most popular of which are coracoclavicular screws [7-8] and hook plates, [9-10] and more recently, tailor-made lateral clavicular plates. Most of the fixation techniques depend on metal work such as plates or wires, while some tend to violate normal structures such as the acromioclavicular joint and also does not address the ligament. The button system, typically used for acromioclavicular joint dislocation, addresses the conoid ligament and also reduces the fracture.
Case History
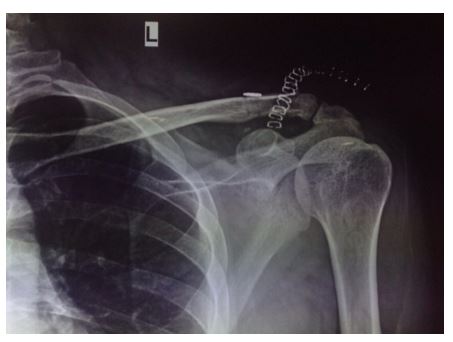
A 46-year old male was involved in a road traffic accident and sustained a displaced left distal clavicle
fracture with a small distal fragment attached to the acromion; this was classified as a Neer Type IIB distal
clavicle fracture (Figure 1). Surgery was performed on the third day after the injury.

Through a vertical incision from the coracoid extending proximally to the clavicle, fracture site was exposed, coracoid was exposed and its base identified and a small window was made to pass Ethibond No 5 suture across the coracoid base.
At the insertion level of the conoid 2cms from the AC joint a drill hole is made with a 2.7 mm drill in the clavicle. Two loops of Ethibond No 5 are looped around the base of coracoid and brought through the hole in the clavicle using suture retriever. Free ends of one Ethibond No 5 is passed on to the two holes of the button, one of the other free end of the Ethibond No 5 is taken out of the drill hole anterior to the clavicle. Fracture is reduced and the through the endobutton is tied and reduction checked under C arm. Additional knots are tied over the button. Wound wash given and closed in layers.
The immediate post-operative radiograph revealed a reduced fracture and well positioned button implant (Figure 2).
The patient was instructed to use an arm sling for 4 weeks and perform gentle range of motion up to shoulder level for that period of time. Full range of motion of the shoulder and strengthening exercises were prescribed after 4 weeks. At 12-week follow-up, the patient was pain-free and had regained full range of movement of the left shoulder.
Discussion
Type II distal clavicle fractures occur medial to (type IIA) or between (type IIB) the coracoclavicular ligaments. Lack of stability from the coracoclavicular ligaments results in displacement superiorly, which requires surgical reduction and fixation for proper healing. There is a high risk of non-union, ranging from 22 to 30% for nonoperative treatment [2,11]. Various techniques have been described for treatment of these fractures, but the ideal method of fixation remains to ascertained [12-13]. This is probably due to the
associated complications of many of these surgical techniques.
Originally designed for syndesmotic injury of the ankle, the Tightrope system has been used for anterior cruciate ligament reconstruction and stabilization of acromioclavicular joint dislocation. The system has been used as an adjunct for closing the coracoclavicular interval in addition to fixation with plates. The so-called ‘snow-shoe’ hold of these buttons on cortical bone enables the implant to withstand cyclic load without cutting out of bone. This type of fixation provides good apposition of the fracture fragments for union by maintaining the reduced coracoclavicular interval. This also allows the injured coracoclavicular ligaments to heal better with anatomical reduction. As the acromioclavicular joint is not violated, complications such as arthrosis are avoided. There is no risk of shoulder impingement as no hardware is placed into the subacromial space as may occur with use of a hook plate. The implant is relatively low profile, and thus obviates the need for a second surgery for its removal. We have modified this technique by using a button on the clavicle and Ethibond No 5 around the coracoid.
The main drawback of this technique is that the coracoid process must be exposed thereby placing the nearby musculocutaneous nerve at risk.
There is a need for fixation method that offers adequate stability for early shoulder mobilization, yet avoids complications associated with conventional fixation methods. The button fixation is a promising option for displaced distal clavicle fractures as a stand-alone fixation.
Conclusion
Distal clavicular fracture due to its unstable nature needs operative fixation. The purpose of fixation is to avoid the deforming forces acting on the fragments which can be done with flexible or rigid fixation. Though function achieved was nearly equal doing a flexible and semirigid fixations, button fixation seems to avoid most of the implant related secondary complications. Further rigid fixations need a major re-surgery for implant removal whereas button fixation, if at all needed implant removal can be done with a simple surgery under local anaesthesia [14].
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!