Biography
Interests
Faroug Ahmed, B. M.1* & Alaa Mohi Edeen Mahmoud2
1Associated Professor, Faculty of Sciences and Technology, Shendi University, Shendi-Sudan
2Medical Student, Faculty of Medicine and Health Sciences, Shendi University, Shendi-Sudan
*Correspondence to: Dr. Faroug Ahmed, B. M., Associated professor, faculty of sciences and technology, Shendi University, Shendi-Sudan.
Copyright © 2019 Dr. Faroug Ahmed, B. M., et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
The oral contraceptive hormones, introduced in 1960, have under gone much modification. The term
“contraception” is defined as the intentional prevention of pregnancy. Contraceptives are therefore
pharmaceuticals or devices that prevent pregnancy. The goal of contraception is to prevent unintended
pregnancy without causing adverse effects and to preserve fertility, when desired. Worldwide, the contraceptive
pills are used by 100 millions of women in child bearing age [1]. Two types of oral contraceptive pills
are available in market, the combined oral contraceptives containing both estrogen and progesterone and
progestin containing only progesterone. The combined oral contraceptive pills are prepared in three different
formulations, i.e. monophasic, biphasic, triphasic depending on the concentration of estrogen and progestin
in menstrual cycle [2].
Estrogens facilitate the growth of the ovarian follicles and increase the motility of the uterine tubes. The estradiol secretion rate is 36μg/dl. Almost estrogen comes from ovary, and there are 2 peaks of secretion; one just before ovulation (380μg/dl) and one during the mid luteal phase (250μg/dl). The principle target organs of progesterone are the uterus, the breasts, and the brain. In men the plasma progesterone level is approximately 0.3ng/mL and in women is 0.9ng/mL [3]. The action of contraceptive pills depending on that estrogen inhibits the release of follicle-stimulating hormone (FSH) and thus suppresses the development of the ovarian follicle. The progesterone inhibits the release of luteinizing hormone (LH) and thus prevents ovulation, and it also makes the cervical mucus less suitable for the passage of sperm. Together they alter the endometrium in such a way as to discourage implantation [4].
All other types of hormonal contraception in current use in the UK are progestogen-only and share many similar features in the terms of mode of action and side effects. Because they don’t contain estrogen, they are extremely safe and can be used if a woman has cardiovascular risk factors [5]. The current mode of progestogen-only contraception are progestogen-only pills, subdermal implant, injectable, hormonesreleasing intrauterine system. Females rats implanted with progesterone gained weight more rapidly than control animals and had an increased proportion of total body fat. Restriction of food intake to control levels demonstrated that the weight changes were not dependent on increased energy intake [6]. In vitro studies have demonstrated that estrogen exerts favorable actions on the endothelium, for instance, stimulating the production of nitric oxide [7] and reducing the expression of adhesion molecules [8]. Moreover, estrogen is capable of promoting in vivo protective actions, such as the decrease of soluble adhesion molecules [9] and reduction of hepatic triglyceride lipase, which degrades HDL (High Density Lipoprotein), stimulating, thus, the production of HDL cholesterol and reducing the production of LDL (Low Density Lipoprotein) cholesterol [10]. Estrogen also affects the cardio vascular (CV) system through its impact on CV risk factors such as the lipid profile. Oral contraceptives (OCs) alter the lipid profile through the genomic pathway, in which estrogen receptor alterations affect hepatic apolipoprotein up regulation [11,12]. Large clinical assays show that the extended use of estrogen associated with progesterone cannot be beneficial and may, also, compromise the efficiency of the autonomic modulation of the heart rate [13].
Some studies show no evidence of unfavorable effects due to estrogenic therapy on autonomic heart rate control with women who practice regular physical training, in the rest condition [14]. Studies report that there are alterations of the metabolism of plasmatic lipids of young, females using oral contraceptives, and that the estrogen and progesterone dosages are related [15]. However, other authors report that low-dose, combined contraceptives reduce the adverse effects of the increases of the total triglyceride and cholesterol serum levels [16].
Santos, et al, 2008 [17], conducted study to detect the influence of oral contraceptive use on lipid levels and cardio-respiratory responses among healthy sedentary women, their study revealed that low doses of estrogen/ progesterone did not affect the aerobic capacity and autonomic modulation in this selected age range. However, it does contribute to modifications of the lipoprotein metabolism related to increases of the total cholesterol and triglycerides levels. Mohammad, et al, 2013 [18], studied the effect of combined oral contraceptive pills on lipid profile, blood pressure and body mass index in women of child bearing age, in family planning department of tertiary referral health care hospitals of Peshawar. They found that contraceptive had significantly elevated lipid profile, blood pressure and body mass index (BMI). Scocco, et al., 2013 [19], studied the effect of different contraceptive drugs on the lipid profile of Brazilian women, authors found that the anti-androgenic progestogen drospirenone was not effective to counterbalance the beneficial effect of the estrogen on the levels of the high density lipoprotein (HDL). Asare et al, 2014 [20], studied the effect of hormonal contraceptives on lipid profile and the risk indices for cardiovascular disease in a ghanaian community, they found that hormonal contraceptive use is associated with significant increases in body mass index, diastolic blood pressure, total cholestrol, low density lipoprotein. Mohamed, et al., 2016 [21], conducted study on impact of using hormonal progestogen only as contraceptive treatment on plasma lipids, their study showed that the levels of plasma total cholesterol, triglycerides and low density lipoprotein increased by using hormonal contraceptives and this increase were directly proportional to the duration of using hormonal contraceptives. Mohammed, et al., 2017 [22], conducted a study to assess the association between body mass index, lipid profiles and total cholesterol among married versus spinster and they found that upper body mass index was inversely associated with high density lipoprotein (HDL) and total glycerides (TG) in the benefit of a spinster. Although the association between BMI and both HDL and TG may be explained by oral contraceptives causing a decrease in apoprotein, cholesterol, high density lipoprotein, triglycerides the case of married women.
Methods
The volunteer women were subjected to two types of measurements:
women in study sample before weighing was wearing light clothing and without shoes. Anthropometric
measurements; weight (nearest 0.1kg), height (nearest 0.5cm) were measured by using standard medical
balance and measuring tape respectively. Body mass index (BMI) was calculated as sample weight (kg)
divided by height (m) squared (kg/m2).
The women were subjected to fasting process about 12 hours before biochemical testing. Total cholesterol
and total triglyceride concentrations were investigated by using the automatic colorimetric enzymatic
method. Also blood pressure was assessed.
SPSS software was used for data analysis and the results were calculated as mean ± standard deviation.
Differences between groups were compared using student’s t-test, considered significant at the 5% level of
probability.
Results
Discussion
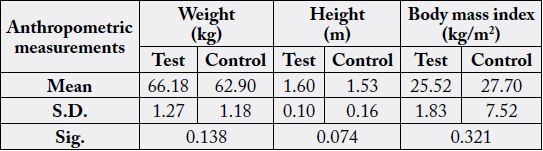
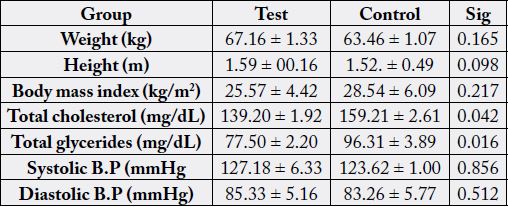
The study did not show a significant difference for body mass index (BMI) (Table 1) although there was
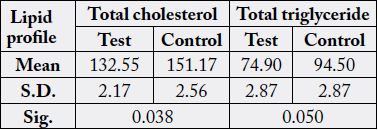
increase in BMI average for control group compared with sample. The study revealed that the averages for
cholesterol and triglycerides for test group were less than that of control group and they showed significant
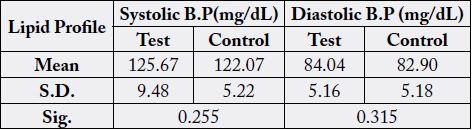
differences (P value = 0.038 and 0.050) respectively, while average of systolic, diastolic blood pressure were
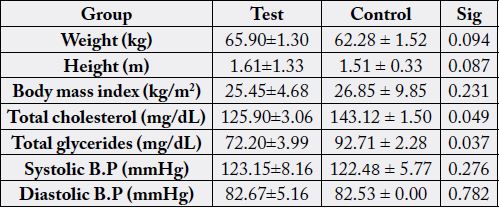
close in both groups and weren’t show significant difference (Tables 2&3 respectively). The same results of
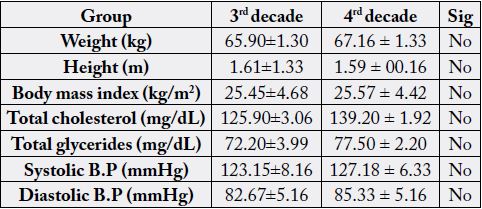
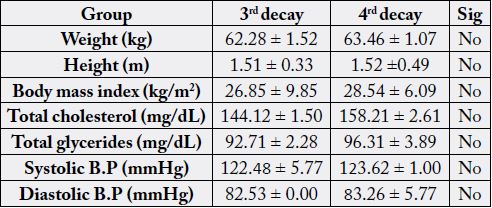
previous measurements were represented when the two groups compared according to age (Tables 4&5). All
values of anthropometric and clinical measurements showed an increase with age progress, but did not show
a significant difference, Tables (6&7). Our findings disagree with that studies conducted by [17, 18, 20, 21]
where their results were revealed that hormonal contraceptive had significant effect on the BMI and some
clinical investigation. On other hand our results were matched with those conducted by [22] which showed
that hormonal contraceptive drugs had no effect on the lipid profile and anthropometric measurements,
and partially it agree with study conducted by [19] which revealed that the progestogen was not effective to
counterbalance the beneficial effect of the estrogen on the levels of the high density lipoprotein (HDL) and
the lipid profile.
Estrogen gains weight through their action on retention fluid and lipogenesis increase. The high oral dose of estrogen can cause fluid retention and symptoms of weight gain or obesity (estrogen obesity). The study was showed that there is no significant difference in anthropometric measurements, although the study questionnaire revealed that some women were gained weight but others loss weight after contraceptive intake. This may be attributed to low concentration of estrogen in the dose (<50mg). Light elevation in blood pressure of test group can be attributed to increase of renine enzyme secretion in the renal under effect of contraceptive. On the other hand, the total cholesterol and triglycerides parameters appeared that hormonal contraceptive had no clear effect on the target measurements. In general, the elevation in measurements value in the benefit of test group could be attributed to absence of estrogen obesity, nutritional status variance and lipoprotein lipase activity.
Conclusion
Many studies have shown that there is a close relationship between hormonal contraceptives and an increase
in body mass index, lipid profile and blood pressure, but this study comes in line with a few of them indicating
that hormonal contraceptives have no significant effect on anthropometric and clinical measurements.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!