Biography
Interests
Harmanjot Kaur1* & Roopjot Kochar2
1Desh Bhagat University, Mandi Gobindgarh, Punjab
2Ayurvedic Nutritionist and administrator, SGS Ayurvedic Diet and Nutrition, Khanna
*Correspondence to: Dr. Harmanjot Kaur, Desh Bhagat University, Mandi Gobindgarh, Punjab.
Copyright © 2019 Dr. Harmanjot Kaur, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Hypertension is one of the most common causes of various diseases in the World and major risk factor for cardiovascular diseases, leading cause of morbidity and mortality. Mental or psychosocial stress is one of the leading risk factor for hypertension which itself is main causative factor for several cardiovascular diseases. The present study has been undertaken on the 130 clinically diagnosed hypertensive patients visiting multispecialty Hospitals in Ludhiana, Punjab. Systolic and diastolic blood pressures (BP) of the subjects were determined using a mercury sphygmomanometer and the stethoscope. A significant (P<0.01) difference was found with respect to male and female systolic blood pressure, however, non significant for diastolic blood pressure of the subjects. Majority of the male subjects were found to be at Stage I (50.70 per cent) degree of Hypertension (BP 140-159 or/90-99mm Hg), whereas, majority of the female subjects were Pre hypertensive (54.24 per cent) i.e. BP 120-139 or / 80-89mmHg. Moreover, a significant (P<0.01) association was found between age and degree of Hypertension of the subjects. 67.60 per cent of male and 45.76 per cent of female subjects were found to live a stressful life. A non significant association was found between various risk factors like stress and sleeping pattern with the degree of hypertension of the subjects.
Introduction
Hypertension (HTN) has become a mainly responsible for global disease burden. It has been considered
as one of the major preventable causes of premature death worldwide especially in developing countries
[1]. Studies have reported up to 60% increase in the numbers of hypertensive adults by the year 2025.
In India, it has assumed epidemic proportions by the year 2015 [2]. WHO predicts that 100 million or
60 per cent of the world’s heart patient will be Indians by the year 2210. Without widespread dietary
improvement Indian heart disease toll has doubled by 2015 [3]. Hypertension is not only an important
risk factor for non-communicable diseases, but also is a major cause of mortality and morbidity all over
the world [4,5]. The prevalence and incidence of hypertension as well as isolated systolic and diastolic
blood pressure is still increasing in most regions [6-8]. Developing countries, especially Asian countries,
are expected to experience the highest increase in hypertension; reports show that about two thirds of
hypertensive patients live in developing countries [9]. About 6.6 million Iranians aged 25 to 65 years old are
suffering from hypertension. Findings show that about 54% of cases of stroke and 47% of cases of coronary
artery disease are attributed to hypertension. The risk of developing coronary heart disease in hypertensive
people was 96% in those without diabetes and 3.23 fold in those with diabetes; the same increasing risk
was observed in case of developing stroke (2.24 and 3.73 fold increase, respectively) [5]. Since, hypertension
is considered asymptomatic; nearly half of the patients are unaware of their disease [10]. Many researchers
believe that major changes in lifestyle behaviors play an important role in the prevalence of hypertension
[11]. Several studies showed that low level of physical activity, being overweight and malnutrition and
being smoker could be associated with increased risk for hypertension even in early adulthood prediction
of hypertension during adolescence [12,13]. Researchers believe that taking antihypertensive medication as
well as lifestyle modification will result in the best therapeutic effect. However, some studies have shown
that when hypertensive patients are informed about their disease, they did not change their lifestyle behavior
[14,15]. So far, a little number of studies has compared the lifestyle behavior among aware and not aware
hypertensive patients, which could be an important step for further treatments [16].
It was reported Hypertension to be present in 29 and 45 per cent myocardial infarction patients of < 40
years and > 40 years of age, respectively [17]. Whereas in another study [3] found 33 per cent of myocardial
patients to be hypertensive and significantly lower prevalence in patients below 40 years of age. Moreover, it
was found 23 per cent of myocardial patients to be hypertensive who were below 40 years of age and 35 per
cent of the subjects were above 40 years of age [18].
A linear association was observed between level of stress and development of hypertension. Persons having
higher mental stress (stress group) were definitely having maximum number of cases of hypertension (59.6
per cent) whereas among No stress group only 12.2 per cent were found hypertensive. It is proven fact that
stress results in immediate sympathetic stimulation with a vasomotor response that result in high-output
state and elevated blood pressure. In another review study ‘Emerging Risk Factors for Atherosclerosis’
observed that five out of 13 studies showed that stress was strongly related with hypertension [19].
Similar observations were made by another investigation in which emotional, sociocultural and occupational stress has been studied in relation with prevalence of hypertension. A number of studies have demonstrated that psychological stress is associated with increases in BP and the development of hypertension [20]. The present study intends to observe the occurrence of stress among the patients of hypertension.
Materials and Methods
The present study has been undertaken on the 130 clinically diagnosed hypertensive patients visiting
multispecialty Hospitals in Ludhiana, Punjab. The selected hypertensive subjects were of age 30 years
and above. Systolic and diastolic blood pressures (BP) of the subjects were determined using a mercury
sphygmomanometer and the stethoscope. Blood pressure was reported as systolic / diastolic mm of Hg. A
set of two readings were recorded each time with help of sphygmomanometer to reduce any type of errors.
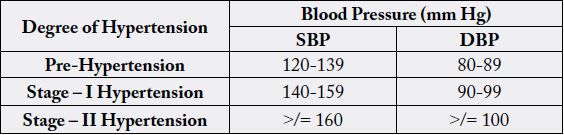
Mean of both the readings was taken as the final blood pressure of the subjects. Furthermore, the degree
of Hypertension was assessed as per WHO, 2003 and JNC VII, 2003 classification. Information regarding
stress status, type of stress and its impact was also recorded for each subject on the pre-printed questionnaire.
Results and Discussion
Blood pressure of the subjects was measured by a mercury sphygmomanometer and a stethoscope. The blood
pressure levels depicted in Table 2 is mean ± standard error values. On an average mean ± standard error
systolic blood pressure of the subjects was recorded as 141.31± 0.54 mm Hg of male and 138.00±0.45 mm
Hg of female subjects. A significant (P<0.01) difference was found between mean systolic blood pressures
of male and female subjects.
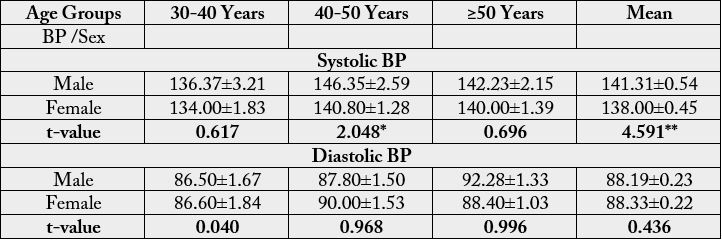
* Significant at P<0.05
** Significant at P<0.01
The mean ± standard error SBP of male subjects at different age groups was recorded as 136.37±3.21, 146.35 ±2.59 and 142.23±2.15mm Hg at age groups 30-40, 40-50 and ≥50 years, respectively. The SBP of female subjects was recorded as 134.00±1.83, 140.80±1.28 and 140.00±1.39mm Hg at age groups 30-40, 40-50 and ≥50 years respectively. Systolic blood pressure of male subjects was found to be higher than that of female subjects at all the age groups. A statistically significant difference has been found between SBP of males and females of 40-50 years of age group. Mean ± standard error diastolic blood pressures of male subjects was recorded as 86.50±1.67, 87.80±1.50 and 92.28±1.33mm Hg, whereas, 86.60±1.84, 90.00±1.53 and 88.40±1.03mm Hg that of female subjects at age group I, II and III, respectively. Moreover, a non significant difference was found between male and female diastolic BP at all the age groups.
The distribution of subjects according to range of blood pressure (Table 3) revealed that majority (48.46 per
cent) of the total subjects had systolic blood pressure between 140-159mm Hg, followed by 35.38 per cent
between 120-139mm Hg. 8.46 per cent of the subjects had SBP ≥160 and 7.69 per cent had SBP considered
as normal (SBP ≤ 120mm Hg).
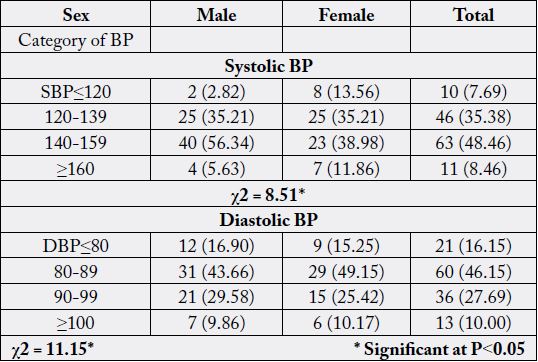
The data on diastolic blood pressure revealed that the maximum (46.15 per cent) per cent of hypertensive subjects had DBP between 80-89mm Hg, followed by 27.69 per cent between 90-99, 16.15 per cent of total subjects had DBP considered as normal (DBP ≤ 80mm Hg) and 10.00 per cent of subjects had DBP ≥100mm Hg. Moreover, a significant (P<0.05) difference was found between male and female with respect to range of blood pressure (SBP and DBP).
More precise distribution of hypertensive subjects on the basis of degree of Hypertension is given in Table 4.
The data revealed that half of the total male subjects (50.70 per cent) were at I stage degree of Hypertension
(140-159 and /or 90-99mm Hg), 11.27 per cent at II stage Hypertension (BP≥160 and / or ≥100mm Hg)
and the remaining 38.03 per cent were found at pre Hypertension (BP120-139 and /or 80-89mm Hg) stage.
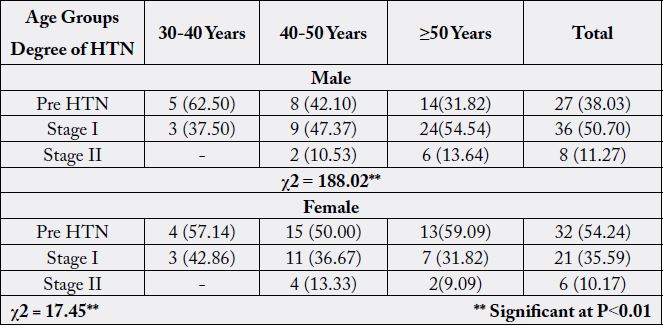
Moreover, degree of Hypertension was found to increase significantly (P<0.01) with the age of male subjects. On the other hand, among female subjects, 54.24 per cent were at pre Hypertension stage, 35.59 per cent at stage I and the remaining 10.17 per cent at stage II degree of Hypertension.
In modern times stress level of human being is increasing continuously and it is responsible directly or
indirectly in the occurrence of the various health related complications. Therefore an attempt has been made
to get information about living status (stress and sleeping pattern) of the subjects.
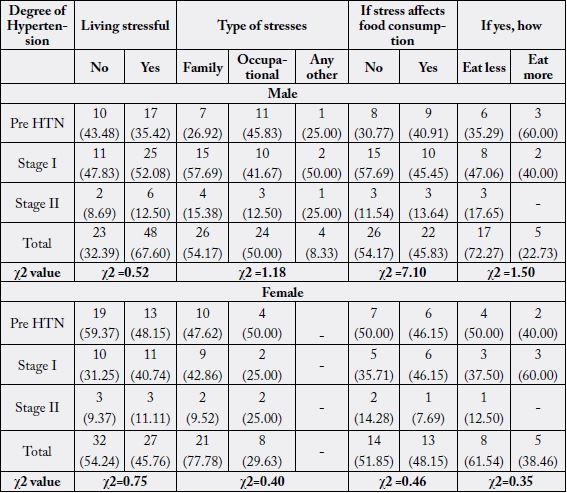
Perusal of the data showed (table 5) that 67.60 per cent of the total male subjects were found to live a
stressful life, out of which, the maximum (52.08 per cent) had stage I degree of Hypertension, followed by
35.42 per cent at pre Hypertension and 12.50 per cent at stage II degree of Hypertension.
Out of the total male subjects living stressful life, 54.17 per cent had family stresses, 50.00 per cent had occupational stress and 8.33 per cent reported some psychological disturbances as the cause of stresses. 45.83 per cent of subjects also reported the effect of stress on food consumption. They were either eating less (72.27 per cent) or more (22.73 per cent) under stressful conditions.
On the other hand, the data about female responses revealed that 45.76 per cent of total subjects were living stressful life, out of which the majority (48.15 per cent) had pre Hypertension, followed by stage I (40.74 per cent) and stage II (11.11 per cent) degree of Hypertension.
Females had more of family stresses (77.78 per cent) than occupational (29.63 per cent) stresses and no one reported any psychological disturbances. Stress had an effect on food consumption of 48.15 per cent of the female subjects too and majority of the females were eating less (61.45 per cent) under stressful conditions.
Thus, 67.60 per cent of the male and 45.76 per cent of female subjects were found to live a stressful life. In male subjects, family (54.17 per cent) and occupational (50.00 per cent) stresses were most common; however, 8.33 per cent also reported some psychological disturbances as the cause of stresses. Females had more of family stresses (77.78 per cent) than occupational (29.63 per cent) stresses and no one reported any psychological disturbances. Stress had an effect on food consumption of both male (45.83 per cent) and female (48.15 per cent) subjects. Majority of the subjects (72.27 per cent of male; 61.54 per cent of female) were eating less under stressful conditions. The subjects at Stage II degree of Hypertension were found to eat less. Moreover, a non significant association was found between living status and degree of Hypertension.
The data on sleeping pattern revealed that 46.48 per cent of the male subjects had sound sleep and 53.52 per
cent were experiencing some sleeping disorders mostly insomnia. 15.79 per cent of the male subjects were
using sleeping pills were (alp salt, tranquillizers etc). On the other hand, out of female subjects, 62.71 per
cent had no sound sleep and 18.92 per cent were taking sleeping pills (meloprax etc).
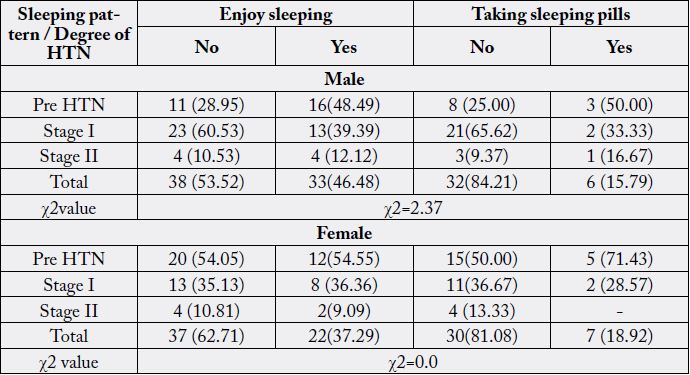
Thus, sleeping pattern revealed that 53.52 per cent of the male and 62.71 per cent of female subjects experienced some sleeping disorders mostly insomnia. Majority of the subjects (84.21 per cent of male; 81.08 per cent of female) were not using sleeping pills. A non significant association was found between degree of Hypertension and sleeping pattern of the hypertensive subjects.
Conclusions
The mean systolic BP of male subjects was found to be 141.31±0.54 and 138.00±0.45mm Hg of female
subjects and moreover the highest SBP was recorded of subjects in the age group 40-50 years. The mean
diastolic BP of male subjects was found to be 88.19±0.23 and 88.33±0.22mm Hg of female subjects.
Moreover, a significant (P<0.01) difference was found with respect to male and female systolic BP, however,
non significant for DBP of the subjects. Majority of the male subjects were found to be at Stage I (50.70
per cent) degree of Hypertension (BP 140-159 or/90-99mm Hg), whereas, majority of the female subjects
were Pre hypertensive (54.24 per cent) i.e. BP 120-139 or / 80-89mmHg. Moreover, a significant (P<0.01)
association was found between age and degree of Hypertension of the subjects. 67.60 per cent of male and
45.76 per cent of female subjects were found to live a stressful life. Among male subjects, family (54.17
per cent) and occupational stresses (50.00 per cent) were common; however, female subjects had more of
family stresses (77.78 per cent). Moreover, majority of the subjects were found to eat less (72.27 per cent of
male; 61.54 per cent of female) under stressful conditions. A non significant association was found between
various risk factors like stress and sleeping pattern with the degree of Hypertension of the subjects.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!