Biography
Interests
Juliana Costa Fernandes1, Ana Maria Keller Jochims2, Ana Beatriz Almeida de Oliveira1, Martine Elisabeth Kienzle Hagen1 & Virgílio José Strasburg1*
1Nutrition Department, Cesan/HCPA, Universidade Federal do Rio Grande do Sul (UFRGS), Brazil
2Nutrition Department, Hospital de Clínicas de Porto Alegre, Brazil
*Correspondence to: Dr. Virgílio José Strasburg, Faculdade de Medicina UFRGS. R. Ramiro Barcelos, 2400, Porto Alegre (RS), Brazil.
Copyright © 2018 Dr. Virgílio José Strasburg, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
The food for collectivities is one of the areas of the nutritionist’s action and comprise food and nutritional care of occasional or defined public. Evaluating the patient’s satisfaction with tools that provide feedback is necessary to have a positive acquisition of improvement for the quality of services provided. The objective of the study was to understand how evaluation tools can improve the acceptance and satisfaction of the pureed diet consumed by patients of a university hospital in the city of Porto Alegre on Brazil. This research is a cross-sectional retrospective descriptive and quantitative study. Secondary data from the Nutrition and Dietetics Service of the hospital were used, referring to the years 2015, 2016 and 2017. A quantitative survey was used to evaluate the lunch meal as a diet received evaluating some sensorial aspects of the meal, besides questions referred to schedule, hygiene and attendance. In the assessment of the acceptance level of the pureed diet was applied an instrument for valuation of consumption through the analysis of food left-over. Data found were inserted on Microsoft Office Excel and were presented in absolute, average and percentage frequencies. The results showing that the eight variables considered in the pureed diet satisfaction survey, the ones that obtained the worst performances were the items assessing sensorial questions of flavour, temperature and variety. The valuation of the acceptance survey established consumption results below the expected for what is considered regular acceptance. In this study the results of the satisfaction survey uphold the assessments found in the acceptance survey and this way was possible to identify that these tools complement each other. It is recommended to carry out similar studies in other hospital institutions as a way to improve the quality of hospital diets in order to increase their consumption.
Introduction
It is necessary to understand physiologically the relationship that occurs between external information and
internal information to understand how the interaction between the need to eat and the human body occurs
[1]. External information corresponds to the characteristics of the food, - taste, texture, variety, nutritional
composition - of the influence of the environment (supply and demand of food, temperature, location, family
context) as well as of religious beliefs, sociocultural aspects and psychological factors (feelings, learning,
habits) [2].
In addition, food can determine different forms of behavior of individuals, since what some define as healthy food in other cultures can be given as a health hazard [3]. In the same way, as in the individual context, these same aspects previously listed are applicable in a context for the provision of meals to healthy or sick groups. For diseased communities, the care of diet therapy is necessary.
Diet therapy serves as a tool for the nutritionist to act in the prevention and treatment of pathologies. However, for the dietary approach be effective, it is essential to establish the best dietary plan, considering the individual needs. In view of this, it is evident that the feeding can also be related to pathologies. According to Demário et al., [4] and Amaral et al., [5] patients loss autonomy during hospitalization its, there being an one-sidedness on the part of the health team that becomes exclusively responsible for the decisions to be made. In addition, the patient in a fragile situation such as hospitalization seeks to compensate through food, making their demands for food and quality service extremely relevant.
The demand for quality services in the food and customer service sector is a major challenge for the Food Units, since it is necessary to satisfy the different nutritional needs of patients with food or nutrient restrictions, combining disease and food preferences [6].
Among the challenges, the food consistency is one of the factors that most affects patient acceptance. According to Stanga et al., [7] this reduction of acceptance occurs mainly because of the change in texture and advises that all those involved in food should be concerned with the different personal tastes and appetites of hospitalized patients. The pureed diet is, the transition between the light diet and the soft diet, is necessary when there is limitation and difficulty in chewing, swallowing and eating food [8].
Hospital diet satisfaction is also correlated with the sensorial properties of meals available, but this perception is modified in the presence of pathologies [9].
In view of all the necessary aspects to offer and guarantee adequate nutrition to hospital patients, it is also necessary to use evaluation instruments in order to identify the acceptance and satisfaction of the diets by the users. Therefore, the objective of the study was to verify the results of the application of instruments of satisfaction and consumption acceptance (food left-over) of pureed diet.
Materials and Methods
This was a cross-sectional, retrospective and quantitative study [10]. Secondary data from patient satisfaction surveys and dietary acceptance surveys were used from the Nutrition and Dietetics Service of a federal public university hospital referring to the years of 2015, 2016 and 2017.
In the satisfaction survey, data from the second half of 2016 and two evaluations were used in 2017. Each study was carried out within a week with an inpatient approach; being applied on one floor per day. A quantitative questionnaire was applied to evaluate the lunch meal considering the total amount, in addition to the study - flavor variables; food temperature; variety of menu; amount; time served; hygiene of utensils; serving of staff; and the nutritionist’s attention - besides the possibility of the interviewees to register suggestions.
For the evaluation of the diet, we considered satisfied patient when the perception of the evaluated variables were classified as “good” and “great”, for the items classified as “bad” and “regular” characterized dissatisfied patient. Patient-specific information, such as age, gender, and associated conditions, was not used.
The acceptance research considers five dietary: soft, pureed, low sodium, diabetes mellitus (DM) and DM without salt. This survey is scheduled to be held twice a year. For each day of the week a type of diet was evaluated in relation to the food left-over. On that day, the menu preparations were served in the thermal dishes of each patient and weighed in the sector where this portioning takes place and after the end of the consumption of the meal by them. The standard of each portion is made according to the dietary prescription prepared by the clinical nutritionist of each patient.
Data were presented in absolute, mean and percentage frequencies. The answers of each item of the satisfaction survey questionnaire and the diet acceptance data were tabulated in the Microsoft Office Excel program.
The research project was approved by the Research Committee of the Faculty of Medicine of the Federal University of Rio Grande do Sul (UFRGS) under no. 34785/2018. The data of the hospital institution were used upon completion of the Term of Commitment for Data Use.
Results
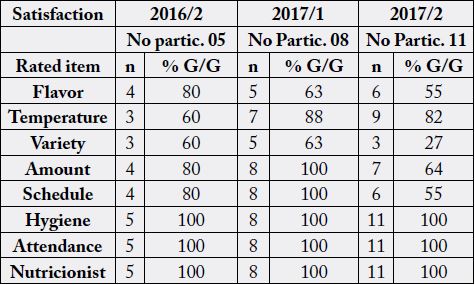
Source: Hospital de Clínicas de Porto Alegre (2018) [11] Note: no partic.= total number of participants; n= total number of survey participants who assessed items as Good or Great; %G/G= percentage of responses evaluated with the options Great or Good;
The sum of participants from the three periods totalled 24 participants. Of the eight variables considered in the satisfaction survey with the patients, the ones that had the worst performances were the items of taste, temperature and variety according to table 1.
Among the evaluated items, the menu variety presented the worst evaluation index by the participants, independent of the semester investigated. There was a gradual and sharp fall of this item over time, reaching values below 30% for good and good responses in the last period.
In this study, there were no negative responses to the care provided by the service, nor to the nutritionist. The work of the nutritionist was efficient for all patients who were interviewed during the three satisfaction surveys performed, since all the answers were good and excellent.
Regarding the item on the temperature of the meal, the worst performance was recorded in the second half of 2016. On the other hand, the items evaluated for hygiene and care reached 100% satisfaction in all evaluations.
In addition to the patient satisfaction survey, there were evaluations of acceptance of dietary intake.
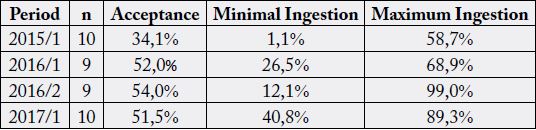
Source: Hospital de Clínicas de Porto Alegre (2018) [11]
The food left-over studies were carried out with patients hospitalized between the 5th and 9th floors.
The hospital usually offers in the same meal rice and beans, meat and garnish. For the pureed diet the meat is shredded chicken with sauce or ground beef with sauce; the garnishes are vegetable or vegetable creams (pumpkin, spinach, carrots) or pasta; the rice is in the pasty form and the beans are only offered the broth.
The findings corroborate with what was specified in the satisfaction survey evaluations where the evaluation of taste, temperature and variety had the worst performances. Another point to consider are the types of food offered especially vegetables and green stuff, which usually have great refusal to feed.
Sensory characteristics of food, especially flavor, are listed as determinants of food consumption, so that food that does not look tasty, pleasant odor and characteristic, with good appearance and texture, will be little consumed.
Discussions
The results found regarding the variety of the menu corroborate with the findings of Ferreira et al. [12],
where the monotony of the menu was indicated with 33% of the reasons for not accepting the diet among
cancer patients.
It is explicit that in order to satisfy the alimentary desires of patients, it is necessary to elaborate menus and this is only up to the dietician [13]. By means of a diversified diet one can reduce the suffering of the pathological picture and hospitalization, avoid and / or reduce nutritional deficiencies, provide individualized and specialized nutritional support, and preparations capable of meeting specific nutritional needs.
In Santos et al. study [14], one of the factors found for the low acceptance of diets was the lack of qualification on the part of the nutritionist professionals, since in order to reach an adequate service that corroborates with the patients’ expectations, constant training and updating.
Cancer and Alzheimer’s disease are pathologies that interfere with food intake. In patients receiving treatment for cancer the side effects of drug therapy often cause symptoms such as inappetence and nausea [12]. In Alzheimer’s disease, there is an inadequate food intake as a result of progressive neurodegeneration that impairs intellectual functions leading to a situation of incapacity and total dependence and dysphagia [15,16].
The results of food temperature obtained in 2017 were similar to the study by Lassen et al. [17] who identified that the temperature item reached 87% satisfaction with the hospital meal served to the patients at lunch.
In this same study, Lassen et al. [17] also indicated the type of care provided as a factor for better adherence to the hospital’s diet by the patients. The British Association for Parenteral and Enteral Nutrition also lists other factors that may negatively influence food intake, such as poor presentation of meals, coincidence of meal times with clinical procedures, lack of consideration by the food service for cultural differences or needs special, communication failures between nursing and the nutrition service and the preparation, transportation and delivery do not ensure the preservation of nutritional content and the palatability of meals [18].
In relation to good dietary acceptance, Lima et al. [19] determined that a meal can be considered of good acceptance when it presents percentage greater than 90%, regular acceptance between 60% and 90% and low acceptance when lower than 60%. In our study, the results were below the expected for what is considered regular acceptance, since this indicator did not exceed 54% considering all periods.
There are studies that have observed that patients have a low food intake not only associated with their pathologies or lack of appetite and taste alterations, but because of the sudden change in habits and dissatisfaction with the hospital environment, type of food options [7], consistency of diet, quantity and quality of food [20].
The study by Souza et al. [21] revealed the disease, lack of appetite, altered taste, difficulty in eating or malabsorption, hospital environment and care as factors compromising acceptance of the hospital diet and which, given this, lead to malnutrition. In addition, there is a dependence on the part of the patients to feed themselves [18]. Corroborating this statement, Santos et al. [22] described that half of the patients needed the help of a relative or companion to eat their meals.
According to Silva et al., [23] the good presentation combining colors, shapes and the disposition of the foods, can contribute to the improvement of the appetite, as well as the monotony of the menus must be avoided. The creativity of menus that appeal to attractive meals and at the same time take into account the needs and expectations of the patient assists in the better acceptance of the hospital diet [21].
Foods such as carrots, tomatoes, cabbage, chayote and yams showed a greater rejection in relation to other foods in the hospital diet [22]. Lassen et al. [17] emphasized in their study that the vast majority of patients do not like vegetables, despite understanding their importance for health.
Kandiah et al. [24] analyzed meal acceptance of 346 patients for four days at lunch, with 36.7% accepting more than half of the meal, 46.2% accepting less than half and 17.1% not accepting the meal offered. Indeed, there were a three times greater risk of non-consumption by the patients once once the food’s consistency was altered.
In the study by Coloço et al. [25] the change of consistency and composition of food were factors that negatively influenced the food acceptance of the patients, since the preparations that advocate this type of diet are difficult to handle in terms of temperature and appearance.
Foods have the purpose of contributing to the recovery and maintenance of nutritional status and meeting the nutritional needs of the patient [4]. In addition, food has been attributed to slowing the suffering caused during hospitalization, since the patient is delimited of his [13]. However, there are few studies in the literature that specifically evaluate the acceptance of oral or restricted diets in the hospital context [26].
According to the 1th Brazilian Consensus on Nutrition and Dysphagia in Hospitalized Elderly [27], the pureed diet is composed of well-cooked foods, in pieces or not, that require little mastication, such as pureed rice, meats and well-cooked chopped vegetables, soft breads and creamy soups and/or pieces of well-cooked vegetables.
The standard of hospital diets is of extreme importance to facilitate the service of nutritionist. There is greater monitoring regarding the amount of food offered, considering the individual characteristics of the diet offered and food consumed, besides making food safety and quality possible [14].
The concern with adequate nutrition of hospitalized patients has been increasing. This is because it is too high the prevalence of malnutrition in hospitalized patients [28]. Therefore, hospitalized patients depend on the diet actually ingested to meet their daily nutritional needs, since when there is no adequate food intake, hospitalization time [29]. The problem of insufficient intake is also associated with an increase in morbidity and mortality, reaching values between 30 and 50% of the hospitalized patients [30].
Some studies indicate that the prevalence of malnutrition among hospitalized patients can vary from 20% to 50% [29,30]. Garcia [13] justified poor feeding as one of the main reasons found for the occurrence of hospital malnutrition. Food is a circumstantial factor for debilitation of the clinical picture of the individual due to sudden food changes that occur from one hour to another, change of daily habits and meal times to which patients are submitted during hospitalization.
Among the limitations of the study was the access to medical records where issues such as present pathologies, gender, age and length of stay could be seen. In addition, it was not possible to measure how much each patient actually consumed each preparation of the menu of pureed diet offered, since the weight of the food was measured together.
Conclusion
Access to a variety of safe and healthy food is a fundamental human right and during hospital stay that right
must be ensured through the food service and individual nutritional care designed to meet the nutritional
needs of patients.
Hospital diets represent an essential tool in the treatment of patients. In view of all the aspects necessary to offer and guarantee adequate nutrition for hospitalized patients, it is necessary to ally food and evaluation instruments in order to identify the acceptance and satisfaction of the diets by the patients.
This study showed that the use and rate of internal evaluation tools may be useful for the diagnosis of acceptance and consumption, identifying the findings of these tools as complementary. The use of the two tools - acceptance and satisfaction - can add together in the improvement of the quality of the services provided by the Nutrition and Dietetics Service of the hospital, as the patient is satisfied with the meal offered, as well as with the hospital environment, food left-over tend to decrease.
Thus, using such resources and developing improvement plans may contribute to improve the effectiveness of patients’ post-meal consumption. It is recommended to carry out similar studies in other hospital institutions as a way to improve the quality of hospital diets in order to increase their consumption.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!