Biography
Interests
Demir Hulya* & Ermis Pınar
Nutrition and Dietetic Department, Yeditepe University, Turkey
*Correspondence to: Dr. Demir Hulya, Nutrition and Dietetic Department, Yeditepe University, Turkey.
Copyright © 2018 Dr. Demir Hulya, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Coffee is one of the most consuming beverages of world. Coffee is owing its effects on health to its compounds; caffeine, diterpene alcohols and chlorogenic acid. Caffeine shows effect as a potential antagonist of adenosine receptors in nerve system. The physiological effects related to caffeine are central nerve system stimulation, metabolism rate acceleration and acute rise on blood pressure. In epidemiologic studies conducted last 30 years the effect of coffee and caffeine consumption on hearth diseases is researched and although it showed coffee has potential of increasing the risk of cardiovascular disease; in cohort studies it is showed that on individuals who consume high amount of coffee, there is no relation between coffee consumption and cardiovascular risks. People often consider coffee has bad effect on health of hearth though lately research results has the opinion of coffee has a strong effect reducing risk of chronic diseases. Because of that, there is need for randomize controlled, prospective and highly provable long termed studies.
Within this scope, this study is conducted between September 15th and December 15th 2017, in Istanbul-Keyifle Yaşam Healthy Nutrition and Diet Advice Center, with women that have body mass index higher than 25kg/m2 between the ages of 18-65 to investigate the effect of coffee consumption to cholesterol LDL and total cholesterol values. As a result of the study, it is found that coffee consumption rate is; related with cholesterol LDL values, not related with total cholesterol level, coffee type, size and amount consumed in a day is related with cholesterol LDL and total cholesterol levels.
Introduction
Coffee is a plant lives in a limited area on world (coffee belt) at after 30 meters from see level. It looks shiny, waxy and grows double leaf. It blooms as jasmine after it becomes ripe. It is from Rubiaceae family. Coffee is gathered from the seeds of red fruits of this family’s one of Coffea type trees. The fruit gets separated from its pulp and rind, occurring seeds get roasted and infused in a granulated form to create one of the most consuming beverages [1]. The ingredients of coffee are as important as its taste. Coffee is a complex drink that includes many compounds as carbohydrates, lipids, nitrous compounds, vitamins, minerals, alcoholoids and phenolic compounds [1,2]. Coffee consumption and its relation with health is examined by observational studies. The epidemiologic studies conducted in the past created worry since there found consumption of coffee and caffeine potentially affects health negative, and over consumption of coffee is related with unhealthy attitudes as smoking and sedentary lifestyle [2,3]. However lately conducted studies gives idea about coffee consumption may act effectively on reducing the risk of some chronic diseases [4,5]. Since old and new studies show contradictory ideas and methodological concerns, there is no absolute statement about coffee’s impacts on health [5].
Coffee is a complex beverage that contains more than 1000 biologically active compounds including caffeine (a strong central nervous system stimulant and bronchodilator). diterpene alcohols (serum cholesterol stimulant) and chlorogenic acid [6]. The caffeine amount in coffee shows difference due to the type, roasting degree and preparing method of coffee. A standard coffee is considered to carry 100mg of caffeine. It is stated that 240ml of infused coffee, which has 14 different specialities, which taken from coffee serving places in America, have between 72-130mg of caffeine [7]. Although, coffee producing is supplied in specific standards, caffeine content of coffee shows difference [7]. Caffeine performs its basic activation as an antagonist of adenosine receptors. Adenosine is a neuromodulator that is synthesized in central nervous system, vascular endothelium, hearth, liver, adipose tissue and muscles and mainly acts role in starting and conducting of sleep. However, caffeine shows opposite effect by connecting adenosine receptors that adenosine can hold on to [8].
Coffee bean compound goes through significant changes during roasting and cooking. Especially during roasting process many reactions create compounds that giving coffee taste [9]. Commercially important 2 types are Coffea arabica Linn. (Arabika) and Coffea canephora Pierre ex Froehner (Robusta). %70 of the coffee producing in the world is type Coffea Arabica. That type of coffee is produced from greenish yellow oval Arabica seeds, it has less caffeine than Robusta and it is more delicious and sweeter aroma than Robusta. Mountain. Robusta coffee creates approximately %30 of the coffee production in the world [9].
It has strong resistance against climate conditions, it is easy and cheap to grow. The coffee gathered from yellowish brown circle Robusta seeds has two times more caffeine than Arabica [10] Depending on the type, in green coffee seeds’ compound there are %50 polysaccharide, %13 protein and %12 lipid. Also, chlorogenic acids, minerals as firstly potassium, manganese, iron and copper, aliphatic acids, trigonelline and caffeine is found [11]. Diabetes mellitus (DM) is a chronic disease that characterized with the genetic or acquired lack of insulin secretion and insulin resistance. There are some studies claiming that decaffeinated coffee reduces the risk of Type 2 DM. Coffee contains chlorogenic magnesium and caffeic acid that has antioxidant effect [12]. Chlorogenic acid helps reducing the absorption of sugar taken from food in intestine therefore it has an effect on reducing insulin-sensitizing. A 240-ml cup of coffee contains the compounds helping to reduce Type 2 DM risk that are 72-130mg of caffeine, 85-420mg of chlorogenic acid and 7mg of magnesium. Researchers showed that every cup of drank per day reduces the risk of Type 2 DM on %7[11]. Also it is accepted that the antioxidants in coffee like chlorogenic acid, could improve glucose metabolism and insulin sensitivity [13]. Diterpenoid alcohols (cafestol and kahweol) are lipids in coffee and they may affect the cholesterol level. Concentration of diterpenoid oil components changes due to the preparing of coffee. It is less than 0.1mg/100ml in filter coffee while it changes between 0.2 and 18mg/100ml in unfiltered coffee [12]. Diterpenoids in unfiltered coffee may increase the LDL cholesterol and decrease the HDL [14].
A meta-analyze study that covers fourteen randomized controlled trial (RCT) reported that consumption of boiled coffee according to the taken amount increases serum total cholesterol and HDL levels while filter coffee increases the serum cholesterol level very few. Increased cholesterol level can increase the incidence and prevalence of coroner heart [15]. In a research where coffee’s effects on serum lipid levels were examined, 107 adults that have normal cholesterol levels were followed for 12 weeks. Coffees were prepared with commonly using filtering and boiling methods and participants were divided in 3 groups in 9 weeks’ period as people who don’t drink coffee, people who daily drink 4-6 cups of filter coffee and people who daily drink 4-6 cups of boiled coffee. While there is a serious increasing of cholesterol level in boiled coffee consuming group, there isn’t observed any reasonable statically difference on LDL cholesterol level [16].
This study is conducted in Istanbul-Keyifle Yaşam Healthy Nutrition and Diet Advice Center, with 100 women that have body mass index higher than 25kg/m2 between the ages of 18-65 to investigate the effect of coffee consumption to cholesterol LDL and total cholesterol values.
Materials and Methods
Universe of the research is, in Istanbul-Keyifle Yaşam Healthy Nutrition and Diet Advice Center between
September 15th and December 15th 2017, where the application of the study is planned. Sample is comprised
of 100 women applied to mentioned advice center, whom have body mass index higher than 25kg/m2.
Data of the study are collected by the general information data gathering form prepared by the researcher and the results of blood tests.
In evaluation the data is firstly classified then necessary codification is made. After the data needed gathered
from assigned sample group by data gathering forms, these data are used in computer environment with
(Statistical Package for the Social Sciences) SPSS 20.0 statistical packaged software. As descriptive statistics
percentage distribution is used in categorical data and Mean±standard deviation is used in continuous
political data. For analyzing categorical data Anova and correlation tests were applied. P<0.05 is accepted
meaningful as statistics [17].
Institute permission is taken. Clinical Researches Ethic Judgment No:745
Results
100 volunteers participated in our study. It is founded that %16 of participants were between the ages of
18-24, %63 were between the ages of 25-40 and %21 were between the ages of 41-60. %3 of the participants
have graduated from primary school, %28 have graduated from high school, %55 are undergraduate and 14
are postgraduate. %57 of the participants is currently working in different institutions and organisations,
%33 is not currently working and %10 is students. %32 of the participants have 1000-2000 TL income per
mount, %19 have 2000-3000 TL income per mount, %20 have 3000-4000 income per mount and %29 have
more than 5000 TL income per mount.
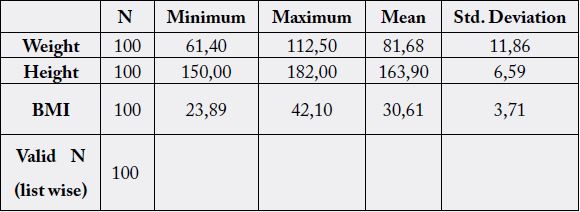
When Table 1 is examined, it can be seen that lowest weight in participants is 61.40kg, highest weight is 112.50kg and average weight is 81.68 and the lowest height is 150cm, highest height is 182cm and average height is 163.90cm.
Minimum body-mass index of participants is 25.98kg/m2, maximum body-mass index is 42.10kg/m2 and mean body-mass index(BMI) is 30.61±3.71kg/m2.
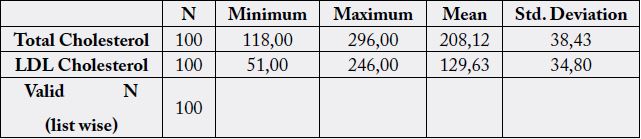
In Table 2 it is showed that, when total cholesterol levels are examined minimum cholesterol level is 118mg/dl, maximum cholesterol level is 296mg/dl and average cholesterol level is 208.12±38.43mg/dl; also when LDL cholesterol levels are examined minimum level is 51mg/dl, maximum LDL cholesterol level is 246mg/dl and mean LDL cholesterol level is 129±34.80mg/dl.
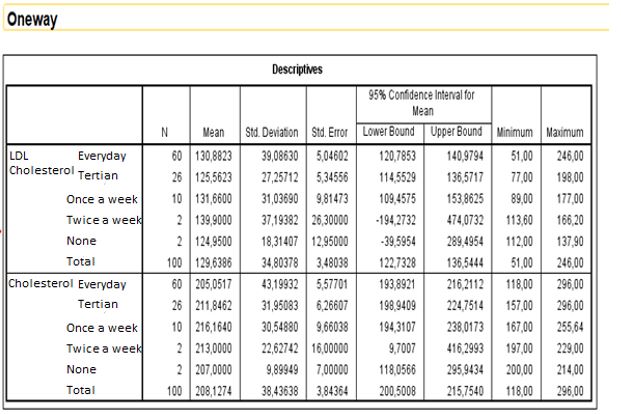
At Table 3 it is shown that, based on everyday consumption range, number of people consuming coffee is 60 and average LDL cholesterol level is 130.88mg/dl, average cholesterol level is 205.05mg/dl. Based on tertian coffee consumption range number of people consuming coffee is 26 and average LDL cholesterol level is 125.56mg/dl, average cholesterol level is 211.84mg/dl. Based on once a week coffee consumption range number of people consuming coffee is 10 and average LDL cholesterol level is 131.66mg/dl, average cholesterol level is 216.16mg/dl. Based on twice a week coffee consumption range number of people consuming coffee is 26 and average LDL cholesterol level is 139.90mg/dl, average cholesterol level is 213.00mg/dl. Number of people who don’t consume coffee is 2 and average LDL cholesterol level is 124.95mg/dl, average cholesterol level is 207.00mg/dl.
There is a relation between coffee consumption frequency and LDL cholesterol level(p=0,00<0,05). People who have high coffee consumption have high LDL cholesterol levels and people who have little coffee consumption have little LDL cholesterol levels.
There is no relation between coffee consumption rate and Total-cholesterol(p=0,899>0,05).
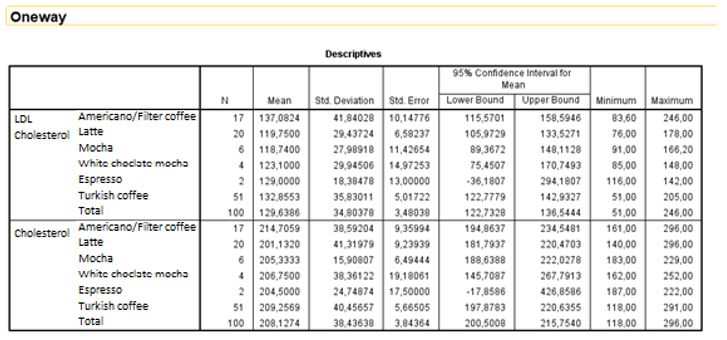
When Table 4 is examined, it can be seen that the number of Americano consumers is 17, mean LDLcholesterol value is 137.08±41.84mg/dl and cholesterol value is 214.70±29.43mg/dl. The number of Latte consumers is 20, mean LDL-cholesterol value is 119.75±29.43mg/dl and cholesterol value is 201.13±27.98mg/dl. The number of Mocha consumers is 6, mean LDL-cholesterol value is 118.74±27.98mg/dl and cholesterol value is 205.33±15.90mg/dl. The number of White Chocolate Mocha consumers is 4, average LDL-cholesterol value is 123.10±29.94mg/dl and cholesterol value is 206.75±38.36mg/dl. The number of Espresso consumers is 2, mean LDL-cholesterol value is 129.63±18.38mg/dl and cholesterol value is 204.50±24.74mg/dl. The number of Turkish coffee consumers is 51, mean LDL-cholesterol value is 132.85±35.83mg/dl and cholesterol value is 209.25±40.45mg/dl.
There is no meaningful difference between coffee type and LDL-cholesterol. There is no meaningful difference between coffee type and cholesterol(p>0.05). But it can be said that preffered coffee type is linked with LDL-cholesterol and cholesterol values. p>0,05. There is no difference. But it can be said that preffered coffee type is linked with LDL-cholesterol and cholesterol values.
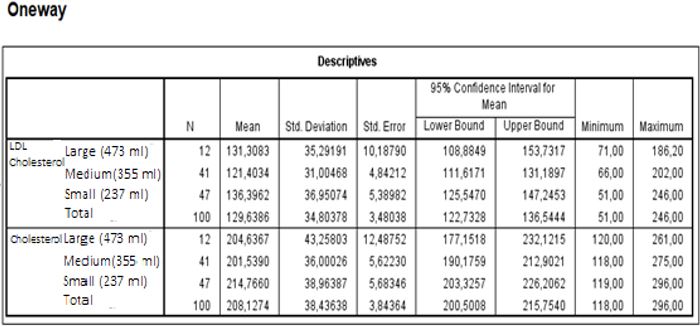
When Table 5 is examined, the number of people consuming Large cup (473ml) coffee is 12, average LDL-cholesterol level is 131.30±35.29 and total cholesterol level is 204.63±43.25. The number of people consuming Medium cup (355ml) coffee is 41, average LDL-cholesterol level is 121.40±31.00 and total cholesterol level is 201.53±36.00. The number of people consuming Small cup (473ml) coffee is 47, average LDL-cholesterol level is 136.39±36.95 and total cholesterol level is 214.76±38.96.
There is no meaningful difference between coffee extent and LDL-cholesterol(p>0.05). There is no meaningful difference between coffee extent and cholesterol(p>0.05). However, it can be said that coffee extent has a link with LDL cholesterol and cholesterol levels.
Discussions
Coffee is a complex drink that includes more than a thousand biologically active compounds as caffeine (a
strong center nervous system stimulant and bronchodilator), diterpene alcohols (serum cholesterol stimulant)
and chlorogenic acid [6]. The caffeine amount in coffee can be change according to; coffee type, roasting
degree and cooking method. Those specialties occur during roasting process. During roasting process many
reactions take place that creates the compounds giving coffee its taste. The compounds of roasted coffee
seeds are classified as volatile compounds and non-volatile compounds. Non-volatile compounds of roasted
coffee and the specialties that compounds give to coffee are these [18]: Caffeine: gives coffee its bitterness,
strength and fullness.
The positive or negative effects of coffee on diseases are still discussed. It is stated that the effect can be change due to the type and consumption amount of consumed coffee. According to that, the lipids of coffee may affect the cholesterol level. Concentration of diterpenoid lipid compounds can change by the preparing method of coffee. It is less than 0.1mg/100ml in filter coffee and it changes between 0.2 and 18mg/100ml in non-filtered coffee [19]. Diterpenoids in non-filtered coffee may increase LDL-cholesterol and decrease HDL [20]. In a meta-analysis research, it is noted that consumption of boiled coffee increases serum total cholesterol and HDL levels due to the consumption amount, the consumption of filter coffee slightly increases serum cholesterol level [21].
There are both studies supporting coffee is protective against cancer and supporting it is not [22]. The effects of coffee consumption health are not limited with the mentioned above and it has been associated with other diseases. For instance, it is indicated that coffee reduces the depression risk known as cardiovascular disease develop risk factor. In a study conducted with 50.739 women a significant decrease of depression risk is detected in women who drink ≥4 cups of coffee daily. Since no difference were observed in people drinking non-caffeinated coffee the cause of change is considered from caffeine [23]. Coffee consumption can be effective on weight control in people with normal weight by increasing lipid oxidation and thermic effect of nutrients. On the other hand, after the consumption of high-caffeinated coffee throb, anxiety and sleep disorders have been observed. High caffeine levels (>750mg/day) increased driving out of calcium and magnesium with urine by negatively affecting urination and bone health. Also, getting caffeine by consuming coffee may lead a sudden increase on heart rate and blood pressure. However, regularly consuming little amount of coffee doesn’t lead to that situation [20]. In a research it is showed that adult on men and women consuming coffee more than 9 cups a day (600-900mg of caffeine) serum homocysteine level (which is a risk factor on heart diseases) is higher than it is on people who don’t consume that amount of coffee [20]. In this study; the effect of coffee consumption rate to total blood cholesterol and LDL cholesterol is evaluated by information gathering data collecting forms and blood analysis of 100 women that applied to ‘‘Keyifle Yaşam Nutrition and Diet Advice Center’’ between the ages of 18-65 and have body-mass index higher than 25. As a result, there are 60 people daily, 26 people on every other day, 10 people once a week, 2 people twice a week and 2 people don’t consume coffee.
Examination results showed there is a relation between coffee consumption rate and LDL-cholesterol and there is no relation between coffee consumption and total cholesterol levels. In a study examining the effect of coffee on serum lipid levels, 107 adults with normal cholesterol levels are followed for 12 weeks. Coffees are prepared with commonly used filtering and boiling methods and in the 9 days’ period participants are split to 3 groups as participants don’t consume coffee, participants daily consuming 4-6 cups of filter coffee and participants daily consuming 4-6 cups of boiled coffee. While there was a significant increase on total cholesterol level of people consuming boiled coffee, there wasn’t observed any statistically meaningful increase on LDL-cholesterol level.
Between not-consumer group and filter coffee consumer group, there haven’t found any meaningful difference on LDL and total cholesterol levels. In a meta-analysis where fourteen randomize-controlled studies were collected, it is founded that boiled coffee consumption increases serum LDL (23mg/dl) and total cholesterol concentration (14mg/dl) linked to its dosage; however, filter coffee consumption slightly effects serum cholesterol (3mg/dl) levels [24].
In this study that 100 women were participated, 17 of the participants consume Americano, 20 of the participants consume Latte, 6 of the participants consume Mocha, 4 of the participants consume White Chocolate Mocha, 2 of the participants consume Espresso and 51 of the participants consume Turkish Coffee. At the end of the study there haven’t found any relation between coffee type and LDL-cholesterol and total cholesterol levels. In a study conducted in Holland Wageningen Agriculture University, it is noted that consumption of non-filtered coffee increases cholesterol level.
In coffee beans, a matter named ‘caffestol’ is found, which increases cholesterol. It is explained that, caffestol occurs when hot water is directly poured on to powdered coffee, when well-milled coffee is boiled in water a few times or when metal filter is used instead of paper filter, like in French Press (a glass container for making coffee, in which hot water is poured onto coffee and then a filter is pushed down into the container to keep the solids at the bottom). It is detected that caffestol passes to the prepared coffee unless paper filter is used [25].
A study that is searching the effect of coffee consumption on serum lipid levels of women in China stated that, daily consumption of 5 grams caffeinated coffee in a monthly base has significant effect on serum lipids [26]. Another research stated that, caffeinated coffee consumption has important effects on total cholesterol, LDL-cholesterol and triglyceride however non-caffeinated coffee doesn’t create such affection. It is reported that, the consumption amount of coffee considerably affects serum lipids in women [27]. In a comparative study, serum cholesterol levels of women consuming coffee more than 200mg daily are 11mg/dl more than non-consuming women [28]. Lately conducted studies showed that serum cholesterol levels are positively related with triglyceride in caffeine-medicine users, however no relation was found in caffeine-medicine users and non-users with total cholesterol or LDL-cholesterol. Due and friends [26] in their study stated that, over caffeine consumption in women might slightly increase HDL cholesterol level. They showed that caffeine increases lipid oxidation in muscles and glycogen mobilization. Lipid increasing effects of coffee consumption showed a possibility for effects on coroner heart health. Case control studies are in the direction of over consumption of coffee has a strong relation with coroner heart disease risk. Updated meta-analysis studies of Prospective studies pointed that medium amount coffee consumption has a slightly reverse effect with paralysis risk. Ingredients of coffee are chlorogenic acids, flavanoids, melanoids, lipid-resoluble compounds and caffeine bioactive molecules. These antioxidants reduce the risk of coroner heart disease. For instance, chlorogenic acide increases body’s antioxidant statute [24,29].
When results are evaluated, different resulting are gathered due to preparing method of coffee. In conclusion of conducted meta-analysis studies, an increase on coroner heart disease risk in people consuming 5 cups or more coffee daily is presumed. Despite the mentioned above, in results of prospective cohort type studies, it can be said that when daily coffee consumption is kept in a moderate level (2-3 cups) it doesn’t lead to coroner heart disease risks [29,30].
Conclusion
As a conclusion of this study which is conducted with 100 women in between the ages of 18-65, whom have
body-mass index(BMI) 25kg/m2 or higher it is found that; coffee consumption rate is related with LDLcholesterol
levels, isn’t related with total cholesterol levels and the type, extent and daily consuming amount
of coffee is not related with LDL-cholesterol and total cholesterol levels.
To sum up, these are the determinations of epidemiologic studies searching for positive or negative effects of coffee, one of the world’s most preferred beverages, on diseases;
• The caffeine amount of coffee may differentiate due to its type, roasting degree and cooking method; these specialties take place during roasting in reactions where the compounds giving coffee taste occur.
• According to that, the concentration of diterpeneoid lipid compounds changes due to preparing method of coffee. Diterpeneoids in non-filtered coffee increases the LDL-cholesterol levels [16].
• Consumption of boiled coffee, based on the consumption amount increases total cholesterol and HDL levels, filter coffee slightly increases serum cholesterol level and increased cholesterol level may increase coroner heart disease incidence and prevalence, also it has the potential of increasing cardiovascular risk [16].
• Besides that, after the consumption of highly caffeinated coffee may lead to sudden increase on heart rate and blood pressure. Throb, anxiety and sleep disorders can be observed. Acute and chronic effects show individual differences in people having or don’t having genetic tendency and it can be harmful in individuals who are hypertensive or who have tendency to hypertension.
The effects of coffee consumption to health are also related with other diseases and it is still an argument of discussion. It is noted that the type, cooking method and consumption amount of coffee can change its affects. Coffee lipids as an Active Factor and coffee has a significant contribute to cholesterol increase. A common methodology and new longer termed and controlled researches that can open way to new findings and developments are needed to be done.
Recommendations
Intake of 2-3 cups/daily of coffee can improve cognitive functioning, the sense of sensation, as well as
digestion. Moreover, the same dosage could be effective against coronary heart diseases, diabetes mellitus,
cancer lines, Parkinsonism, and Alzheimer’s disease. Risks associated with its excessive consumption involve
insomnia, coronary complexities, and some others. Health disparities related to coffee consumption are
often attributed to the consumption of an excess amount of caffeine or allied components present in its lipid
fraction. Different processing techniques could be applied to remove such challenging components in order
to minimize the associated risks.
Several studies over the past decade have shown a link between coffee and cholesterol. Coffee oils (known as diterpenes) such as cafestol and kahweol are to blame. Coffee oils are naturally found in caffeinated and decaffeinated coffee. Caffeine is a stimulant. Too much can cause jitters, insomnia, headaches, upset stomach, and anxiety. Some people are particularly sensitive to the effects of caffeine. These people should want to limit how much coffee they drink, or switch to decaffeinated.
The intake of coffee especially unfiltered coffee is contributed significantly to the increase in Total Cholesterol, LDL-Cholesterol, and the changes were related to the level of intake. it may be better to drink the filter coffee to get less cholesterol. Also, if you have a heart problem, you should drink coffee more carefully to get less damage than a cafein.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!