Biography
Interests
Zainab Hussain
Food Service Dietitian at SFC, THI, Pakistan
*Correspondence to: Zainab Hussain, Food Service Dietitian at Safe Food Caterers (SFC), Tabba Heart Institute (THI), Web Committee Chair, Pakistan Nutrition and Dietetic Society (PNDS), Pakistan.
Copyright © 2018 Zainab Hussain. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Peanut Allergy
Peanut allergy, considered as one of the severe food allergy, is an immune reaction to proteins or small
molecules called haptens in peanuts and the allergy is far different from that to nut or legume allergy. The
allergy occurs as the immune system mistakenly identifies peanuts as a harmful invader.
Many foods share homologous proteins therefore sensitization to one food can result in positive tests or clinical reactivity to related foods developing multiple foods sensitization sometimes leading to the development of allergy symptoms.
Prevalence of Peanut Allergy
In children approximately 90% of hypersensitivity reactions are caused by milk, peanuts, eggs, wheat and
soybeans whereas, in adults, fish, shellfish, tree nuts and peanuts account for approximately 85% of allergic
reaction.
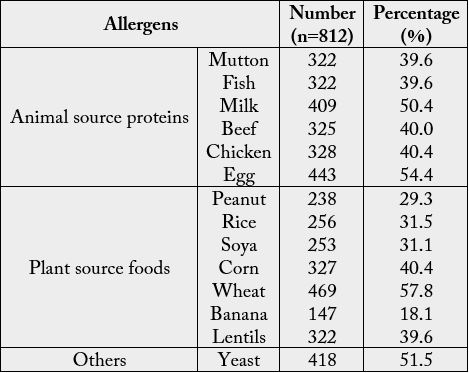
Pakistan is no exception to this increasing global issue, but no studies are available in literature showing prevalence of sensitivity to various foods consumed as part of diet in Pakistan. According to a study done in Islamabad in 2016 revealed the following statistics [1]:
Origin of Peanuts
Peanuts, taxonomically classified as Arachis hypogaea, from the family Leguminosae; also known as earthnut
or groundnut, is a small plant grown mainly for its edible seeds in most tropical areas of Africa, India, Brazil,
South U.S.A. and Australia, and then exported to other countries. Various types of peanuts are found which
show differences in the relative amount of fatty acids contained in its oil. Groundnuts are the world’s fourth
largest source of fixed oil [1].
Proteins in Peanuts
Peanuts contain good amounts of some essential amino acids like they contain high levels of arginine and histidine. The remaining amino acids are also present in substantial quantities except methionine, tryptophan and cystine which are low in quantities [2].
Moreover, Ara H1 is a seed storage protein in peanuts. It plays an important role in peanut allergic reactions. Several studies have demonstrated that the protein fraction of the cotyledon is the allergenic portion of the peanut. Ara H1 makes up 12% to 16% of the total protein in peanut extracts and is classified as a major peanut allergen because it provokes sensitization in 35% to 95% of patients with this allergy [3].
This protein is a very potent allergen and it causes a severe reaction. The symptoms can be redness or edema, itching usually around the mouth and throat, diarrhea, stomach cramps, nausea or vomiting, coronary artery spasm or even anaphylaxis.
Another aspect is that cooking methods can affect the allergenicity of peanut like roasted peanuts have higher levels of Ara H1 than fried and boiled ones [4].
Diagnosis of Peanut Allergy
Diagnosis of food allergies, including peanut allergy, begins with a medical history and physical examination.
Milk allergy can be diagnosed by the person’s history of allergic reactions, skin prick test (SPT), patch test and measurement of milk protein specific serum immunoglobulin E (IgE or sIgE). Confirmation of the allergy can be done by double-blind, placebo-controlled food challenges, conducted by an allergy specialist.
A skin prick test, sometimes called a puncture or scratch test, is used to check for immediate allergic reactions. This test is usually done to identify allergies to pollen, different foods etc. In adults, the test is usually done on the forearm. They sometimes tell erroneous results, telling that you are not allergic to certain food, even if you are, that is why one should not completely rely on those results [5].
Signs and Symptoms of Peanut Allergy
The severity of the allergy varies from person to person, and exposure can increase sensitization. For those
with a milder form of the allergy, a reaction which makes the throat feel like cotton may occur. Subjects
allergic to tree nut can experience asthma, skin rashes, itchy throat, swollen eyes. The most severe reaction
can lead to anaphylaxis.
The raw nut protein usually causes a more severe reaction than the oil, and extra roasting or processing can reduce the allergic reaction.
This allergy tends to be lifelong; studies have shown that only about 9% of children outgrow their tree nut allergy [6].
Treatment of Peanut Allergy
Currently strict avoidance of the allergenic food and ready access to self-injectable epinephrine is the
standard of care for food allergy. Clinical trials for peanut allergy using the anti-1gE therapy to prevent
circulating 1gE from binding to effector cells are underway. Peanut allergy can be devastating as reactions
range from urticaria to severe anaphylactic shock and death. The only preventive measure for peanut allergy
is strict avoidance [1].
Maternal Hypersensitivity
There is conflicting evidence on whether maternal diet during pregnancy has any effect on development of
allergies due to a lack of good studies. A 2010 systematic review of clinical research indicated that there is
insufficient evidence for whether maternal peanut exposure, or early consumption of peanuts by children,
affects sensitivity for peanut allergy [7].
Other Similar Peanut Allergies
Walnut, pecan and hazelnut form a group of strongly cross-reactive tree nuts while hazelnut, cashew, Brazil
nut, pistachio and almond are moderately cross-reactive tree nuts [8].
Legumes are a family of foods including peas, beans, lentils and peanuts. Children (or adults) who are
sensitive may also have skin reactions to legumes in their dried form used in craft activities e.g. collages
using lentils [9].
Conclusion
Peanut allergy is one of the most dangerous food allergies, and one of the least likely to be outgrown. Here,
we conclude that, atopic individuals are more susceptible to having multiple foods sensitization. This study
is an attempt to evaluate the gravity of food hypersensitivity in Pakistan and to better anticipate and address
this rising community and health service burden. Further research is required to estimate a correlation
between SPT based sensitization and development of symptomatic food allergy. Moreover, Immunotherapy
treatments are being developed for tree nut allergy. Immunotherapy involves attempts to reduce or eliminate
allergic sensitivity by repeated exposure. This active research concept involves swallowing small amounts
of peanuts, holding a peanut product under the tongue - sublingual immunotherapy - skin patches or
injections. None of these are considered ready for use in people outside of carefully conducted trials. In those
with mild peanut allergies, gradually eating more and more peanuts resulted in at least some short-term
benefits. Due to the amount of evidence being small and the high rate of adverse effects, this is not currently
recommended as treatment. Sublingual immunotherapy involves putting gradually increasing doses of an
allergy extract under a person’s tongue. The extract is then either spat or swallowed. It is not currently
recommended as treatment; however, it is being studied. Epicutaneous immunotherapy involves giving the
allergen through a patch. Trials are ongoing [10].
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!