Biography
Interests
Khin-Htun, S.* & Ko, B.
Department of Medicine, University of Nottingham, UK
*Correspondence to: Dr. Khin-Htun, S., Department of Medicine, University of Nottingham, UK.
Copyright © 2019 Dr. Khin-Htun, S., et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background
Clinical reasoning (CR) is a recursive, multidimensional, and complex process involving informal and
formal strategies for the analysis and evaluation of patients’ information. CR skills are traditionally acquired
through the experiential learning of undergraduate (UG) students as they progress through the curriculum,
particularly as they rotate through clinical placements. Recently there has been an acknowledgement of the
need to explicitly teach CR. The University of Nottingham (UoN) aimed to introduce a vertically integrated
CR theme. The opportunity provided by this development was used to develop, implement and evaluate this
CR curriculum.
Well-developed CR skills are important for doctors to allow them to reach diagnoses for their patients. The
course structure for medicine at UoN consists of a pre-clinical phase and a clinical phase, with three separate
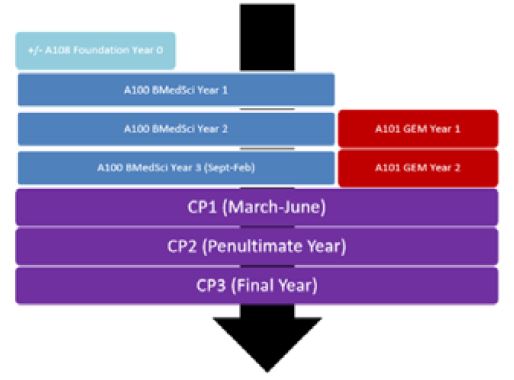
entry routes converging by the start of the clinical phase. There are the five and six-year UG courses (A100
and A108) and the graduate-entry, four-year course (A101). For all three tracks, the educational objective
is the same: to acquire the knowledge, skills, and behaviour to allow graduates to practice as new doctors on
the foundation training programme with the Bachelor of Medicine/Bachelor of Surgery degree. In addition,
all students on the five-year and six-year courses obtain a BMedSci degree. Figure 1 summarises the course
structure of the UoN medical degree, and how the different pathways interlink to conclude in qualification.
Methodology
This study is aimed at evaluating whether Clinical Reasoning is Explicitly Embedded into the University
of Nottingham medicine curriculum. The first author was involved in all the steps of the curriculum design
process as part of the curriculum committee. The first author monitored all of the planning processes,
implementation decisions, and creation of evaluation tools for measuring how effectively the curriculum
elements achieved the CR goals. The UoN CR curriculum is dynamic with the researcher maintaining
involvement in efforts to change some of the CR components, while other changes occurred without
intervention. This study followed a moving target to identify where and how CR curriculum changes were
taking place. The philosophy and design of this study is essentially descriptive and associative and not
necessarily rigorously comparative.
Evaluating whether CR is successfully embedded into the curriculum is a key part of this study. One of the principles of curriculum evaluation is gathering data on what is occurring in the curriculum. The following is the overall development, the setting up, the development of educational resources, the planning, implementation, and evaluation of the educational interventions and the redesigning of the whole CR Curriculum, as it happened:
The UoN CR curriculum operated on a six-step approach to curriculum development for medical education
by Kern, Thomas, Howard, and Bass (1998). This six-step approach consisted of the following steps: (a)
problem identification and general assessment; (b) needs assessment of targeted learners; (c) goals and
objectives; (d) educational strategies; (e) implementation; and (f) evaluation and feedback (see Figure 2).
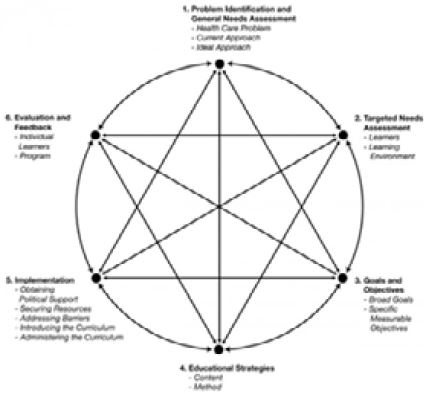
This approach was dynamic, interactive and continuous in nature, and did not necessarily proceed in sequence. Progress was often made on two or more steps simultaneously, with progress on one step influencing progress on another. The curriculum development never truly ends but is cyclical, as demonstrated by figure 2 above. The curriculum evolves, based upon evaluation results, changes in resources, changes in targeted learners, and changes in the material requiring mastery [1].
In the case of UoN, problem identification and general assessment was done by literature review. Extensive research regarding the last forty years of CR data led to the development of this CR curriculum at UoN.
For needs assessment, the curriculum developers explored the current knowledge, beliefs, and attitudes of UoN medical students on CR by interviewing them.
In terms of goals and objectives, the development of CR curriculum was aimed at creating or updating the standards of higher medical education and modernization of the integrated curriculum. The goals and objectives were aligned with the General Medical Council (GMC) ‘Outcomes for graduates’ from Tomorrow’s Doctors (2015) [2], ‘Developing a framework for generic professional capabilities, a Public consultation’ (2017) [3], Scottish Deans’ Medical Education Group SDMEG (2008) [4]. the Scottish Doctor: Learning Outcomes for the Medical UG in Scotland, The Royal College of General Practitioners (RCGP) 2015: Core Curriculum Statement [5], The Royal college of Surgeons (England), and ‘The curriculum framework for the surgical Care Practitioner (SCP) (2014) [6].
Educational strategies were piloted in each year and evaluated as students moved through the curriculum in order to determine the best methods for implementation of this curriculum. After the pilot phase, the curriculum resources were formally introduced into the UG curriculum.
As for implementation, “Educational Principles that Guide the UG Curriculum” by Dennick and Garrud (2008) [7] provided an outline of the educational principles underpinning the medical curriculum, using a curriculum framework created from a synthesis of a variety of medical educational sources.
Regarding evaluation and feedback, the four-level Kirkpatrick model [8] was used in this curriculum. Level 1 of the Kirkpatrick model is the reaction. This is a measurement of the learner’s feelings and opinions about the course just completed. This first level involves perceptions of the learners (i.e. staff members) who are undergoing training. Level 2 consists of the learning event and the measurements of what was learned as a result of the learning event. Level 3 is the measurement of the behavioural changes that occurred as a result of the learning event. Level 4 is the results for the organisation - for example, the measurement of the overall impact of an innovation on the institutional environment. Levels 3 and 4 could not be evaluated since the students are not yet working in clinical areas and thus cannot transfer their knowledge.
Results
The figure 3 and table 1 will signpost places where CR is embedded and how it is linked to the existing
programme. Mapping this vertical curriculum and identifying which element is explicit and which is implicit
in the final curriculum model shows CR where it is embedded.
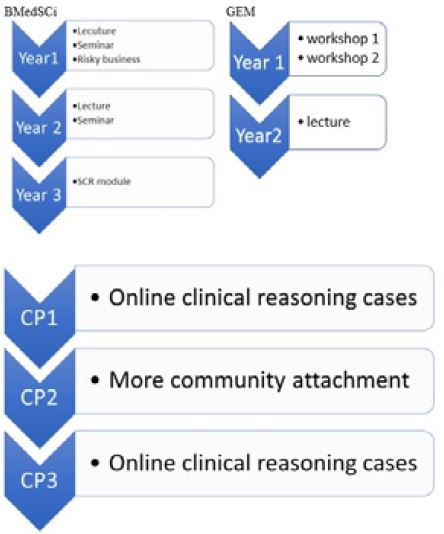
Table 1: Final Curriculum Model
This new revised curriculum as a whole is intended to integrate and make learning clinically relevant. Case
studies are used throughout the week to inform teaching and rounded off by a case study workshop at the
end of the week to engage the students in deep learning.
One Introductory Lecture
One Seminar
Optional Module: Risky Business
One Lecture
One Seminar
Scientific Basis of CR is delivered to all year 3 students who joined Life Sciences Homebase Modules. The
purpose of this module is to facilitate experiential learning and CR. It is Patient centred course and the aim
is that all participate in the problem solving.
Problem-based learning (PBL) sessions
CR is explicitly taught in the following:
• CR workshops
• Clinical skills ‘exploring symptoms’ workshops
• Evidence-based medicine lectures
In order to get the consistency between all different sites, training the teachers “How to Teach CR in work
place” is started. We make sure all the clinical teachers from different sites have new competencies to teach
these skills.
A graded series of case scenarios based on core clinical presentations will be provided on-line each month as
CR Tests. These regular on-line clinical cases will be provided to develop thinking about CR.
The researcher has also proposed to introduce ‘symptom-to-diagnosis approach teachings’ in place of previous ‘individual pathology and diseases approach teachings’.
Significant new changes are taking place within the exam across all 3 clinical phases and the knowledge
paper is shifted from examining simple recall of knowledge to integration, interpretation and application
of knowledge. OSCE stations will now increasingly move away from the traditional checklist marking to
a hybrid domain marking scheme or domain based model. CR domain will be examined in almost every
station. The duration and number of OSCE stations are changed and it is an opportunity to become more
integrated and system based rather than uni-dimensional system based stations.
o ABC of CR is published [9]
o Established clinical-reasoning.org website so that the students and the teachers could see the teaching
materials [10]
o Faculty training program will continue (The first author)
Conclusion
The main focus of this study was “Evaluating whether CR was embedded into in the UG curriculum at the
University of Nottingham”
Because of these recent interventions, UoN BMedSci is a more integrated course with more clinically relevant experience, case studies and a patient centred approach along with an increased focus on dissection studies. The science component of the BMedSci was not dropped, but was reinforced by an increase in the CR activity. The GEM course with its CR components was still continuing. CR has been successfully implemented for the clinical years and in a faculty development programme for clinical teachers. These are the evidence that CR is embedded vertically throughout UoN UG curriculum.
Even a well-conceived curriculum that has been carefully maintained as health problems and societal needs evolve [1]. Therefore, it is very important to maintain, enhance and prolong the life of this CR curriculum. A curriculum that is static will gradually decline and die. A successful curriculum must be continually developing. Therefore, it needs never ending reviewing.
Finally, that curriculum will be reinforced by the students’ clinical experience, and which will prepare them more effectively for qualification, to develop the skills of CR so that ultimately patient safety is enhanced.
Recommendations for Practice
The authors first recommend that CR teaching curriculum be used as a way to enhance the CR of students.
Even though the literature on the effectiveness of a formal curriculum in developing CR has not been
established, this study extends the support for its effectiveness. The clinical training of students should have
explicit and implicit CR components designed to enhance students’ CR. This also requires teachers to have
new competencies to teach CR skills and the CR faculty development programme should be implemented.
List of Abbreviations

Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!