Biography
Interests
Arunima Datta1, Prathama Guha2* & Subpiramaniyam Sivakumar3
1Dept. of Psychology, Netaji Subhas Chandra Bose Cancer Research Institute, Kolkata, West Bengal, India
2Institute of Psychiatry, Kolkata, West Bengal, India
3Associate Professor, Dept of Bioenvironmental Energy, College of Natural Resource & Life Science, Pusan National
University, Miryang-si, Republic of Korea
*Correspondence to: Dr. Prathama Guha, Institute of Psychiatry, Kolkata, West Bengal, India.
Copyright © 2019 Dr. Prathama Guha, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Cognitive changes among diagnosed breast cancer patients are often attributed to chemotherapy, without considering other comorbid factors.
The present study evaluates the impact of chemotherapy on cognitive function among breast cancer patients those who were undergoing chemotherapy. The comparison was determined by the variation of the effect of DNA mechanism due to different types of chemo-medicine.
51 women with non-metastatic breast cancer those under-going chemotherapy were evaluated into two groups on the basis their chemo medicine: combination with 5-fluorouracil or without 5-fluorouracil. Cognitive impairment was signified with an assessment of validated Kolkata Cognitive Battery.
The relationship between cognitive function and different combination of chemotherapy along with dosages variation was compared between Group-1 and Group-2. Parsons’s “r” correlation revealed in changes of chemo medicine combination with 5FU Medicine: chemo cycle, verbal fluency and time, calculation, word memory Trail 1 and Trail 2 was significantly correlated with variation in chemo medicine. In the group of Chemo medicine combination Without 5FUMedicine: chemo cycle, verbal fluency, Object naming and time, MSE. However, in group 1, verbal fluency, object naming, delayed word memory and delayed word memory recognition were also significantly correlated with dosages variation of chemo-medicine.
In the present study result depicted, variation of chemo-medicine and dosages was associated with poor cognitive function in patients receiving chemotherapy.
Introduction
During and after the chemotherapy treatment some of the cancer patients reported adverse effects of
cognitive function such as impaired memory, attention, speed processing, verbal fluency and other different
basic cognitive activities [1]. These effects were researched by many scientists through eliciting neurotoxicity
of chemotherapy [2]. In 1990, some of the researchers had studied the effect of cognitive function in breast
cancer patients who had received chemotherapy. These studies reflected that patients scored lower than
expected cognitive performance on the neuropsychological assessment. Almost of 10 years of research had
proved the impact of chemotherapy on cognitive function without any reasonable doubt. In first generation
of the studies are observational and cross-sectional. So, the obtained results were ongoing and longitudinal.
Many perspective studies revealed, cognitive deficit found before taking adjuvant chemotherapy due to these
deficits had been transit, induced by surgery and general anesthesia [3]. However, other studies researched
baseline status before neo adjuvant chemotherapy compared with untreated breast cancer patients. There
cognitive deficit was seen 21% and 30% among patients with untreated breast cancer [4]. On other side,
most of the studies had found no evidence of cognitive deterioration among patients who were undergoing
chemotherapy by using methodologically sound large scale. In the majority of perspective studies cognitive
changes had been seen in some of limited cognitive domains (Sharon M. Castellino et al. 2014). Generally,
15%-25% of patients seemed to be affected. Recently, a meta-analytical and neurological studies had
presented, after taking chemotherapy treatment among patients with breast cancer cognitive deficits are on
average. Still, the researchers had 6 comparisons between subjective complaints and objective neurological
assessments. Some of the patients complained the cognitive changes which are not prominent in neurological
assessment. Subjective complain of cognitive deficits are strongly correlated with depression, anxiety or other
neurological assessment [5]. Even in recent studies had found that subjective cognitive complains are more
correlated with depressive symptoms rather than do-main specific neurological assessment [6]. In 2016,
researchers conducted a study among patients with breast cancer and age matched healthy control group in
comparing cognitive performance before and after chemotherapy. There was shaded light on the problem
of cancer-related cognitive impairment (CRCI). CRCI might be related with disease and it’s treatment
including chemotherapy, hormonal therapy, surgery and radiation [7].
In India, there is not any study about effect of chemotherapy on cognitive function. So, we are unable to establish any study related in West Bengal. We hypothesized that self-reported cognitive difficulties, that is, perceived cognitive impairment, assessed via Kolkata Cognitive Battery (KCB) total score, would be more prevalent among patients with breast cancer those who were undergoing chemotherapy. The score of cognitive functions was researched according to the variation chemo medicine and dosage with single component compared with more than one. Secondly, cognitive function was revised as per reaction of DNA mechanism of each medicine.
Methods and Methodology
It was an observational study using validated tools and structured face to face interview.
This study was conducted at two different tertiary hospitals in Kolkata, situated in eastern India, between
May 2017 to August 2017. Early non metastatic breast cancer female participants between age group of
30-60 years, who had at least eight years of formal education were included, after applying specific inclusion
and exclusion criteria.
The researchers had approached 236 non metastatic breast cancer patients undergoing chemotherapy; 86
(65.56%) agreed to participate in the study. Among them, women who had previous history of psychiatric
disorders (N=35), recurrence of cancer (N=34), or who were unable to give information and/or could not
understand or read Bengali, the language spoken by the majority in this part of India (N=30) were excluded
from the study, resulting in a total of 51 study participants.
On the basis of mechanism of action of chemo medicine, they were divided into two groups: group 1 (N=31) who got chemo medicine with combination of 5FU i.e. DNA modifying agent in conjugation with antimetabolite. Another one was group 2 (N= 20) who got chemo medicine with combination of other than 5FU i.e. metabolic inhibitor with DNA modifying agent. All the patients were given the cognitive function test by using validated tools: Kolkata Cognitive Battery. Inclusion and exclusion criteria are given below.
Following were the inclusion and exclusion criteria
Age between 30 to 60 years
Diagnosed patients with early non metastatic breast cancer
Patients undergoing neo adjuvant chemotherapy
Willing to participate in the study
Minimum eight years of formal education
No history of past mental illness
Inability to understand or read Bengali language
Demographic data were collected from all the groups of the study population, followed by administration
of tests in a single interview.
A semi structured proforma was developed to record the sociodemographic and clinical details of the study
subjects. Informed consent was obtained from all participants in writing according to the format laid down
by the Indian Council for Medical Research (ICMR), the apex body governing research in India [8].
Neurological assessment was conducted by using Kolkata Cognitive Battery.This battery consisted of
category based on verbal fluency test, a 15 item version of the object naming test, mental status examination,
calculation, word memory task, delayed word memory task, delayed word memory recognition task andvisual
construction. This battery has already been used and validated by Syamal Kumar Das et al. the patients were
affected by sever, moderate or slight cognitive impairment based on KCB scores [9].
Informed consent was obtained from all participants in writing according to the format laid down by the
Indian Council for Medical Research (ICMR), the apex body governing research in India [8].
Written informed consent was obtained from all participants. Study protocol was approved by Ethical
Committee of institutions. Demographic data were collected via interview using the semistructured
proforma. After dividing two groups by experienced oncologist, they were given the KCB.
SPSS program version 21 was used for compilation and analysis of data. Descriptive statistics were calculated
as the mean±standard deviation of age and frequency of demographic factors was tabulated according to
relationship status, residence, education, occupation and per capita family income. The relationship between
chemo-medicine and score of cognitive assessment was computed using the Spearman’s rho correlation
coefficient. Statistical significance was defined at p<0.05.
Results
Table 1 shows the prevalence of cognitive function according to sociodemographic and clinicopathological
factors
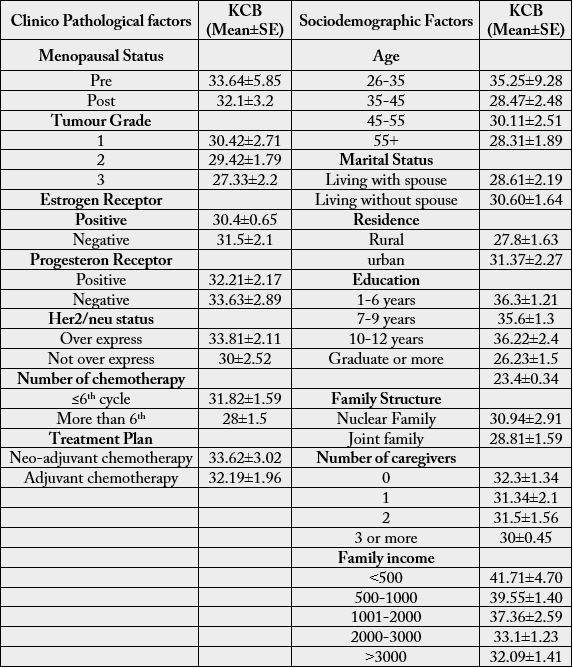
While mentioning the demographic distribution of the studied patients, 47.5% among them were urban people while 52.5% were from rural areas. Age ranges were between 26 to over 55 yrs. Percentage of Patients were lowest (5%) among 26-35 yrs. and highest (42%) among 35-45 years. age group. Among studied patients 62% were living with their spouse and rest of part living alone. Highest percentage(62%) of patients were below high level of school educated. While mentioning cilinicopathological factors, it had been seen that, 58% of patients reported positive estrogen receptors while 53% of patients were with negative progesterone receptors. Human epidermal growth factor receptor 2 was expressed among 58% of patients. 63% of patients was diagnosed with ductal carcinoma. In case of treatment history, 69% of patients were undergoing neoadjuvant chemotherapy along with 61% patients already took more than 6th number of cycle chemotherapy.
In case of other medical illness, 47% of patients were with sugar. (Figure-1)

Table 1 showed prevalence of cognitive function according to sociodemographic and clinicopathological factors. Following the results of table, it had been seen, following clinic-pathological factors such as Menopausal status (pre and post), tumor grade (1,2, or 3), estrogen (positive or negative) & progesterone receptor status (positive or negative), Her2/neu status (positive and negative), type of treatment (adjuvant or neoadjuvant) was not significantly associated with cognitive function. While number of chemo cycle (≤6th cycle and More than 6th) was significantly associated with cognitive function.
According to results of table 1, it had been found, sociodemographic factors such as age, education, residency, family structure is not significantly associated with cognitive function. On the opposite side, family income variation was significantly associated with cognitive function.
Table 2 represents the prevalence of cognitive function according to different combination of chemo medicine. After going through, result had indicated, those patients were undergoing chemotherapy which was consist of 5FU combination medicine, they scored very low (specially, verbal fluency, delayed word memory recognition and word memory task) in the objective assessment rather than those took without combination of 5FU.
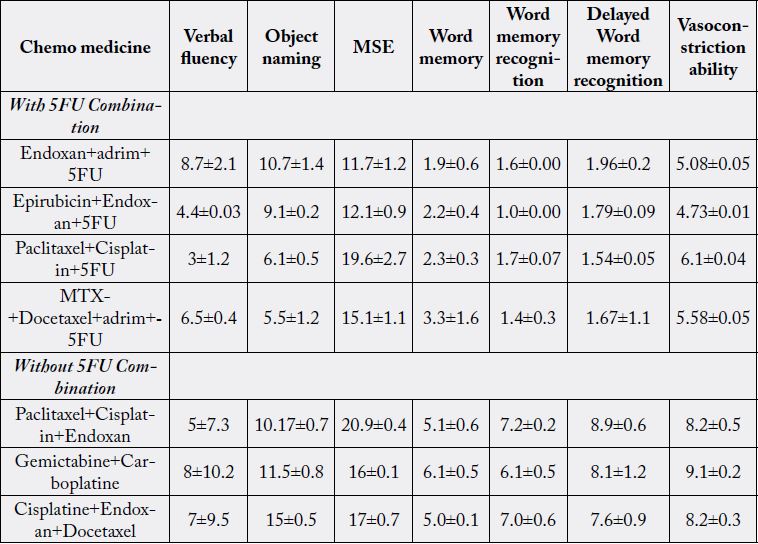
Table 3 represents effect of doses variation according to different combination of medicine. If focused on with combination of 5FU and its dosage variation it could be seen, verbal fluency (1.4(.99-1.81), object naming [1.94(1.81-2.06)], word memory task [.1(.11-10.99)], delayed word memory recognition [.25(.17- 3.49)*] and visuo-construction ability [.51(.39-7.15)*] is significantly associated with dosages variation.
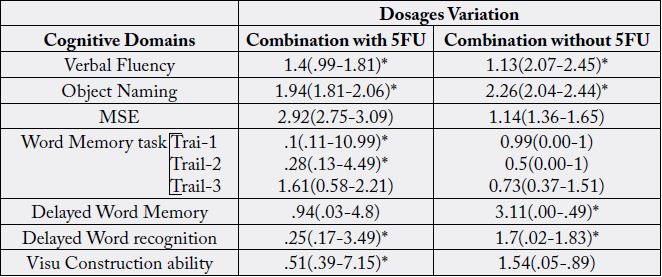
In combination without 5FU, there dosages variation significantly associated with verbal fluency [1.13(2.07- 2.45)*], objection naming [2.26(2.04-2.44)*], word memory recognition [3.11(.00-.49)*] and delayed word memory recognition [1.7(.02-1.83)*].
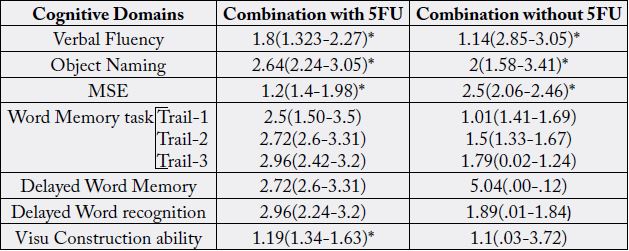
Chemo medicine combination With 5FU
Medicine: chemocycle, verbal fluency and time, calculation, word memory Trail 1 and Trail 2 was significantly correlated with variation in chemo medicine.
Chemo medicine combination Without 5FU
Medicine: chemocycle, verbal fluency, Object naming and time, MSE.
Discussion
The present studies that only address cognitive performance in a cross-sectional manner on the basis of
impact of different chemo-medicine on cognitive function. Possible difference had been determined on the
basis of effect of DNA mechanism of combination of each medicine. To get around these limitations of the
patients’ investigation, investigators have begun to conduct studies that perform assessment of cognitive
functionamong mentioned two groups. The result of present study had reported, in initial condition
during period of chemotherapy, impairment in cognitive function was not significantly affected. In some
of longitudinal studies had reported some of cognitive impairment such as memory, executive function
after following their treatment but in short -term case of treatment did not find cognitive changes [10].
Chemotherapy related cognitive changes is known adverse effect among breast cancer those who are under
chemotherapy. Unfortunately, this type of cognitive complained was not clinically proved. Similarly, some
of researchers had worked over women breast cancer patients who were receiving adjuvant and neoadjuvant
chemotherapy. The authors ultimately found that a patient’s anxiety, depression and low mood is significantly
associated with subjective cognitive function but it was not elicited in neurological assessment [11]. Endocrine
factors may influence objective neurological testing performance after chemotherapy [12]. In a longitudinal
study of breast cancer patients undergoing chemotherapy for early breast cancer patients, menopause
was associated with some decline in cognitive performance following chemotherapy and it was proved
in neurological assessment (Tager FA et al. 2010). This result was contradicted with another prospective
study of women receiving adjuvant chemotherapy. In their study, they had predicted, menopausal symptoms
correlated with quality of life scores but not cognitive performance, as it was determined by high-sensitivity
cognitive screen [13].
Apart from this, objective study is supported with Jonna. E. Fardell (2012) [14] research entitled : “cognitive impairment caused by oxiliplantin and 5- fluorouracil chemotherapy are ameliorated by physical activity”. Studies in women with breast cancer have demonstrated that chemotherapy can have a negative impact on cognitive performance. The results of the present study reported, 5- fluorouracil (5FU) chemotherapy agents had created a negative impact on memory, verbal fluency and calculation. This result is supported with Jenna E (2012) [15]. But, it had been seen, scores of verbal fluency was low in both case those who receive chemotherapy with combination of 5FU regimens and those who not.
The hypothesis of a dosage response relationship between chemotherapy and cognitive impairment in breast cancer patients was confirmed by Collins et al [16]. after controlling baseline performance along with a patient’s age, education mood they found that cognitive function rapidly worsens with cumulative chemotherapy.
Our study had contradicted with Giffard et al [17]. reported that because of life threatening cancer and its treatment both also may involve many stressful events and suffering from psychiatric symptoms such as PTSD, anxiety and depression. These symptoms are known to effect on cognition. A relationship between hypocampal atrophy and deficit in episodic autobiographical memory retrieval was suggested which could reflect of exposure to negative events with cumulative stress.
Chemotherapy can improve prospects for long-term survival after a cancer diagnosis, but it turns survival after a cancer diagnosis, but it may also be associated with long-term toxicity including possibility of cognitive dysfunction. Pharmacologic treatments do not have related cognitive function, clinical guidelines are needed for assessment and management of chemotherapy related cognitive dysfunction.
Therefore, from this study it has been suggested in many cases, chemotherapy medicines are given in combination which means a patient gets two or more than two medicine at the same time which is known as chemotherapy regimens. So, dependency on regimens is not only individual cause of cognitive impairment.
Conclusion
In the present study we have investigated correlated factors for cognitive impairment, comorbidity factors of
the two conditions and it had found there sociodemographic as well as clinical factors were similar among
the three conditions through an exploratory way. Among the correlated factors, in case of dempgraphic and
clinical factor was not associated with cognitive dysfunction. Considering the moderate level of decline and
increased risk factor adverse outcome among those with cognitive impairment, it could better be suggested
that patients with evaluated a proper psychological intervention to give a better quality of life.
Limitations of the Study
This study has its limitations. It was conducted on a relatively small sample size. Most patients belonged to
lower socioeconomic strata and had lesser number of years in terms of formal education, hence it cannot be
said to be representative of all Indian women. No follow up was carried out except for a single sitting with
breast cancer patients to look into their major concerns of life. Finally, we did not look into the possible
protective factors against depression, and more specifically, impaired cognitive performance in cancer
patients. We hope to address these issues in future studies.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!