Biography
Interests
Meron Kibru1*, Fekadu Aga2, Wubareg Seifu3, Beza Tamirat4 & Tadele Kinati5
1College of Medicine and Health Sciences, Midwifery Department, Clinical Midwifery Unit, Jigjiga University, Jigjiga, Ethiopia
2Addis Ababa University College of Health Science School of Allied Health Sciences, Department of Nursing and
Midwifery, Ethiopia
3College of Medicine and Health Sciences, Public Health Department, Epidemiology and Biostatistics Unit, Jigjiga University, Jigjiga, Ethiopia
4College of Medicine and Health Sciences, Public Health Department, Reproductive Health and Nutrition Unit, Jigjiga University, Jigjiga, Ethiopia
5College of Health Sciences, Nursing Department, Salale University, Ethiopia
*Correspondence to: Dr. Meron Kibru, College of Medicine and Health Sciences, Midwifery Department, Clinical Midwifery Unit, Jigjiga University, Jigjiga, Ethiopia.
Copyright © 2019 Dr. Meron Kibru, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Optimum utilization of antenatal care often depends on pregnant women’s perception of provider’s
caring behaviors. In Ethiopia around 74.4% of women do not receive the recommended antenatal care. Despite this, there was no any study conducted in the health facilities of the Ethiopian
Somali Regional State to investigate the client’s perception of the caring behavior of midwives in
the antenatal care clinics. Therefore, this study was conducted to assess the antenatal care client’s
perception of caring behavior of midwives in Faafan Zone, Ethiopian-Somali Regional State.
An institutional based cross sectional study was conducted among 384 pregnant women who came
for antenatal care service within the nine randomly selected health centers from March to April
in 2015. Data were collected through face-to-face exit interview using a pretested and structured
questionnaire. Data analysis was done using SPSS version 20 software package and odds ratio
with 95% confidence interval was estimated using multivariable logistic regression to identify
independent predictors of the client’s perception of midwives caring behavior.
The overall rating of positive perception was 48.7%. The highest score from the caring behavior items
based on their mean were “treat me as an individual (4.44±0.683)” and “point out the things about
me and my condition(4.41±0.683)” were clients scored for their positive perception. Educational
level, age, number of family members and pregnancy related illness were significant predictor of
client’s negative perception of midwives caring behaviors.
The result reveals that most antenatal care attending mothers have negative perception towards
to the caring behavior of midwives. Thus, examining items with negative clients’ perception will
enable midwives to identify the defects in midwifery care and to establish applicable adjustment.
Furthermore, there is a need to conduct a large scale professional caring behavior assessment for the
midwives to identify the measurable gaps at the national level.
Introduction
Pregnancy is considered as a phase in life that makes great demands on the women’s ability to adapt and
adjust physically, psychologically and socially [1]. While most pregnancies and births are uneventful,
all pregnancies are at risk. Around 15% of all pregnant women develop a potentially life-threatening
complication that calls for skilled care and some will require a major obstetrical intervention to survive [2].
It’s believed that this complication should be overcome by early detection of abnormalities and treatment
during pregnancy. Antenatal care (ANC) is the maternal care during pregnancy that every pregnant women
needs for a better outcome. It is an important determinant of safe motherhood and key strategy for reducing
maternal morbidity and mortality [3]. Antenatal care is the key entry point of a pregnant woman to receive
broad range of health promotion and preventive services which promote the health of the mother and the
baby [4].
Client satisfaction with the care provided is an important element of quality care, often determining patient’s willingness to comply with treatment recommendations, thus influencing effectiveness of care [5]. Utilization of antenatal care often depends on pregnant women’s perception of care provider’s caring behaviors. The World Health Organization (WHO) has recommended a minimum of four antenatal care visits to ensure the well-being of mothers and newborns [6]. During these visits, women should receive at least a minimum care package, and be monitored for warning signs of problems during their pregnancy.
Around 23% of the population found in the Ethiopia Somali regional state is in reproductive age with 4.8% of total fertility rate [6]. The Ethiopian Demographic and Surveillance (EDHS) 2011 showed that 74.4% of women did not receive ANC [7]. This may be related with the mother’s perception towards the care given at the health institution and also the providers may not give them enough attention which may leads to poor client-provider communication. So the pregnant mother’s may refrain from visiting the health institution for antenatal care services.
So far no study has been conducted in any of the health facilities of Ethiopia Somali Region to investigate client’s perception of the caring behavior of midwives in ante natal clinic, including the challenges and problems are experienced or how they are handled, if any. The study was designed to analyze and explain the antenatal client’s perception about midwives caring behavior. Finding of the study will help for the health care providers and institutions to address the gaps in midwives caring behaviors during antenatal care. Furthermore, improving caring behavior of midwives at antenatal care clinics would not only contribute to the health of mothers and their babies, but also to expand the knowledge base of the midwifery profession.
Methods and Materials
The Ethiopian Somali regional state has nine zones, 68 woredas (districts) and 4 city councils. Potential
health service coverage of the region is estimated to be 70-73%. Currently there are ten hospitals and 142
health centers in the region. At present there are around 679 midwives who work in hospitals and health
centers in the region. The study was conducted in Fafaan Zone which is located 628Km from the capital
city Addis Ababa in the Ethiopian Somali Regional State from January to May 2015. Fafaan zone have 8
woreda, one city council and 29 health centers. According to the projections based on the 2007 Population
and Housing Census conducted by the Central Statistical Authority (CSA) (we need citation here!), the
total population of Faafan zone is 1,154,390 and of which 54.98% are in reproductive age group.
An institutional based cross-sectional study was conducted in Fafaan zone among randomly selected pregnant
women. The sample size for the study was determined using a single population proportion formula with the
following assumptions: Proportion of pregnant mothers satisfied with the midwifes caring behaviour to be
50%, margin of sampling error tolerated- 5%, critical value at 95% confidence interval of certainty (1.96)
and 10% non-response rate making the final sample size of 422 pregnant women attending ANC. Study
participants were selected systematically from nine governmental health centers in the study area. There were 29 health centers in Faafan zone and from these 9 of them were selected through a lottery method. Preliminary
assessment was conducted to estimate the total number of pregnant women attending ANC prior to the
study period in each of the selected heath centers. The sample size was proportionally allocated to the health
institutions based on the total number of pregnant mothers visiting per day to seek antenatal care service.
Each pregnant mother was selected and interviewed every one interval which was determined by statistical
formula until the desired sample size was achieved for the respective health institutions.
The data were collected using structured and pretested interview questionnaires. A structured questionnaire
was used to collect data on the socio-demographic characteristics, pregnancy related information, and
midwives caring behavior assessment with Likert scale modified and adapted from Jean Watson’s Caring
Behavior Assessment Tool (CAT) (we need citation here). Data collectors were given three day training on
the questionnaires and interviewing techniques. The questionnaires have been translated from English into
the local language, Somaligna and again back translated to English to check consistency and accuracy of
translation. The questionnaires were pre-tested before the actual data collection. Additional modifications
were made to the questionnaire in terms of in terminologies and formatting based on the pretest findings.
The supervisors checked each completed questionnaire and principal investigator monitored the overall
quality of the data collection. Operationally, care is the provision of what is necessary for the health, welfare,
maintenance, and protection, caring behavior it is how the midwife behaves or acts to provide an essential
care for someone who needs it, midwife is a person qualified to deliver babies and to care for women before,
during, and after child birth. The mother’s perception of midwives caring behavior was measured using a
48-item Likert scale with ratings ranging from 1= strongly disagree to 5=strongly disagree. The mean score
was calculated and those who scored above the mean were considered as having positive perception towards
caring behavior of midwives during ANC.
After data collection, each questionnaire was checked for completeness and code was given. Data were entered,
cleaned and explored for outliers, missing values and analyzed using SPSS version 20 software. Descriptive
statistics like frequency tables, graphs were used to describe the study variables. Bivariate binary logistic
regression analysis was used to see the existence of association between dependent and independent variables.
95% CI and p- value less than 0.05 were used as cut of point to see their level of statistical significance. To
control the effect of confounding variables and to identify predictors of the client’s perceptions of midwives
caring behavior, step wise multiple logistic regression analysis was used. Ethical clearance was obtained from
the Department of Nursing and Midwifery at Addis Ababa University. Permission paper was also obtained
from Ethiopian Somali regional and Woreda health bureaus. Similarly after explaining the purpose of the
study, verbal informed consent was also obtained from each study participants while the study subjects right
to refuse was respected. The confidentiality of the information obtained was kept through anonymous data
collection and aggregately analyzing and reporting the findings.
Results
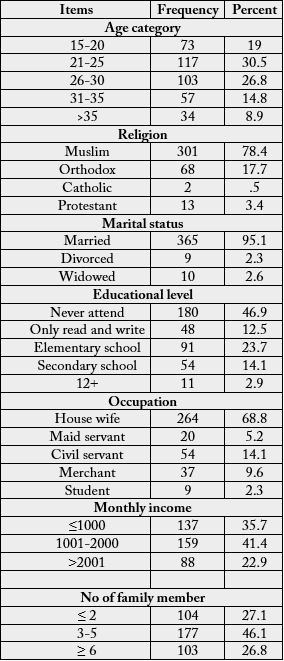
A total of 384 women respond to the questioner which makes a 90.0% response rate. Most (30.5%) of the
women were within the age group of 21 to 25 years with a mean age of the respondents being 26.64± 6.0(SD)
years. Majority (95.1%) were married at the time of data collection. Majority (78.4%) of the respondents
were Muslims in their religion and most (46.9%) of the respondents never attend school at all. Majorities
(68.8%) of the respondents were house wives followed by students (2.3%). The mean monthly income of the
respondents was 1671.61 ±1267(SD) Ethiopian Birr (Table 1).
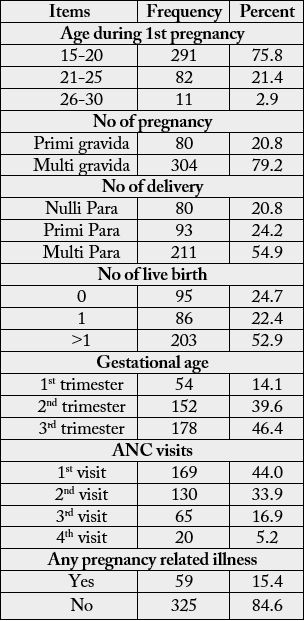
Majority (75.8%) of the mothers have their first pregnancy at the age of 15-20 years. Out of the respondent
(20.8%) of them were primigravida whereas most (54.9%) of the respondents had more than one delivery.
During the course of data collection, most (46.4%) were found in third trimester. Most (44%) of the mothers
were on their first antenatal visit (Table 2).
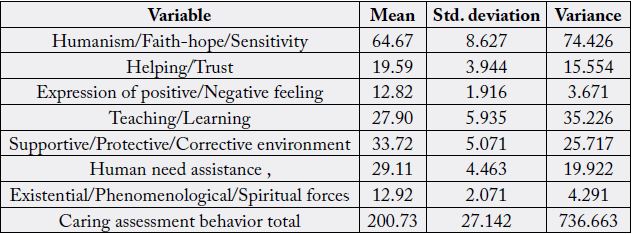
The mean score value for the humanism subscale of the CAT was 64.67 (SD 8.627) while the overall total
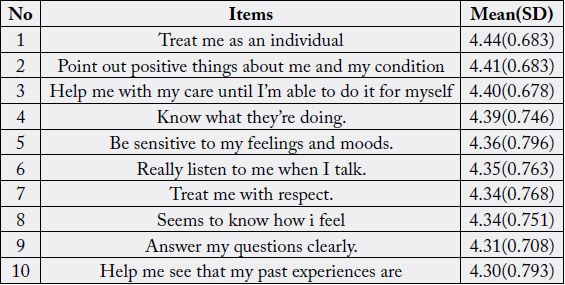
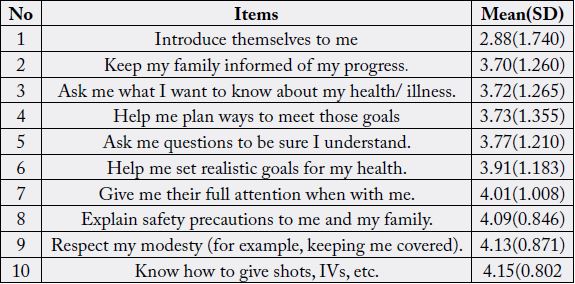
mean score of the CAT was 200.7 (SD 27.14) (Table 3). On the basis of a single item analysis, participant
mean scores on caring behavior were calculated, with a range that fell between 2.88 and 4.44. The range
of mean scores of the top 10 caring behaviors was ranked in terms of most important and fell in a narrow
range (4.30 to 4.44). The range of mean scores for the 10 caring behaviors ranked as least important was
considerably wider (2.88 to 4.15) (Table 4). Five of the top 10 important items for caring behaviors, ranked
first, second, fourth, fifth, and seventh, corresponded with humanism, faith-hope, and sensitivity subscales.
Four of the 10 least important items for caring behaviors, ranked third, fourth, fifth, and sixth, correspond
with the teaching learning sub scale (Table 5).
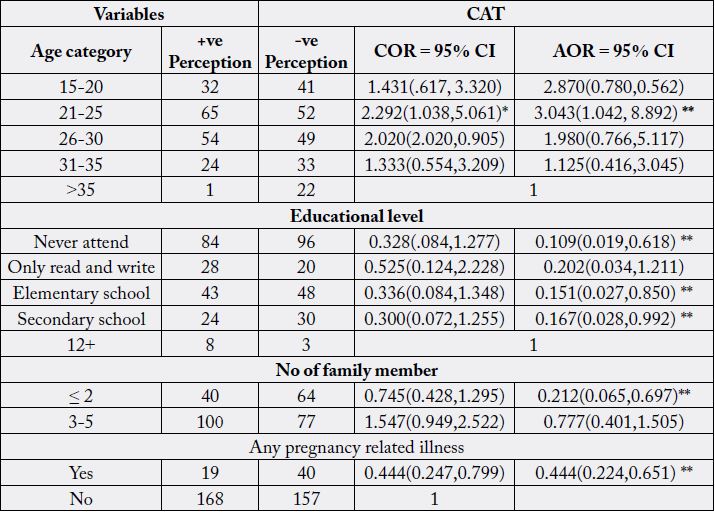
Mothers with the age of (21-25 years) were three times more likely to have positive perception of midwives
caring behaviors than mothers with other age groups [AOR=3.043, 95% CI (1.042, 8.892); p-value ≤ 0.05].
Mothers who never attended school were nine times less likely to have positive perception than those who
have completed 12 grade education and above after controlling the confounders [AOR=0.109, 95% CI
(0.019, 0.61)]. Likewise, mothers who had elementary school education level were five times less likely to
have positive perception on the caring behavior of midwives than those who had 12 and above education
level [AOR=0.151, 95% CI (0.027,0.850)]. Mothers with less than three family members were five times less likely to have positive perception with the caring behavior than those who had greater than seven family
members [AOR = 0.212, 95% CI (0.065, 0.697)]. Among the pregnancy related information pregnancy
related illness shows to have a significant association with mothers’ perception of the caring behavior of
midwives, those who have pregnancy related illnesses were two times less likely to have positive perception
than those who have no pregnancy related illnesses. [AOR= 0.444, 95% CI (0.224, 0.651)] (Table 6).
Discussion
Client’s satisfaction with midwifery care is considered as an important factor in explaining clients’ perceptions
of service quality on midwifery profession. According to O’Connor and colleagues, the patient’s perspective
is a meaningful indicator of health services quality and may, in fact, represent the most important perspective
[8].
Satisfied client usually trust their health care providers, and as a return they comply with medical and nursing recommendations. Then, eventually, the client’s physical and psychological healing process is enhanced and at the same time, they disseminate their experiences to others which increase the number of clients who uses the services. If not satisfied the reverse may happen.
In present study 51.3% of mothers have negative perception about caring behavior that was provided by the midwives. Among the CAT items “treat me as an individual (mean sore = 4.44)” and “point out the things about me and my condition (mean sore = 4.41)” which belongs to humanism/faith /hope/sensitivity scored highest this could be caused, since ANC needs a passionate and caring service this categories of items consists items related with giving faith, hope and sensitivity and “introduce themselves to me (mean sore = 2.88)” belongs to helping/trust scored the lowest as single item this also may resulted from most midwives had not the habit of the introducing themselves to the clients but clients need it as a way to trust their providers. Humanism/faith/hope/sensitivity (64.97±8.627) and supportive/protective/corrective environment (33.72±5.071) rated highest as a subscale.
A study conducted in South Africa states the abuse of antenatal mothers by the midwives as a notable theme [9]. The findings of the same study illustrated that the midwives had excellent theoretical knowledge of caring, but some of them did not display caring behavior during clinical practice [9]. In the finding of our study, mothers who never attend school found to have a significant positive perception of midwifery caring behavior. These mothers probably have taken for granted any behavior displayed by the midwives as they may not have the knowhow of caring behavior of midwives.
In study at hand, mother with the age of (21-25 years) found to have a significant positive perception of midwives caring behavior. However, religion, occupation, marital status, age of mother seemed to be irrelevant in clients’ perception on caring behavior of midwives. These implies that clients with medium age group have noble perspective of the care delivered by the midwives and among the pregnancy related information pregnancy related illness were one of the indicator for caring behavior of midwives as perceived by the clients which found to have a significant association with midwives caring behavior, these implies that those who have pregnancy related illness needs extra care and comfort and midwives should be curious with these mothers.
In another descriptive study that asked mothers who had uncomplicated vaginal births to rate behaviors of their nurses behaviors in the human needs assistance subscale, which included items such as “help me with my care until I’m able to do it for myself ”, “give my treatments and medication on time (mean sore = 4.94),” and “check my condition closely,” were perceived as the most caring [10].
Since this study participants were mother who attend at ANC the behaviors in the Humanism/Faith-hope/ Sensitivity subscale, which include items like “treat me as an individual (mean sore = 4.44)”, “point out the things about me and my condition (mean sore = 4.41)”,“Help me with my care until I’m able to do it for myself ’(mean sore = 4.40)” were perceived as most caring; Whereas “introduce themselves to me (mean sore = 2.88)”, ‘keep my family informed of my progress (mean sore = 3.70)” and “ask me what I wanted to know about my health/illness (mean sore = 3.72)” were considered as less cared.
This study has the following strength: The study utilized a valid and standardized instrument (CAT), the study is the first in its kind in midwifery, so it will create a way for further investigation and also has a high response rate. Despite this strength it has the following limitation: Since it was an exit interview the response may have bias and also pregnant mothers who did not come to the health center were not include because the study was conducted only in health centers [11-20].
Conclusion and Recommendation
The results are useful in their own and in similar settings because they can be used by staff midwives to
improve practice in various ways. The result revels that most clients had negative perceptions of midwives
caring behaviors. Those mothers who came with pregnancy related illness is one of the indicators for the
negative perception about midwives caring behavior. Thus, examining items with negative clients’ perception
will enable midwives to identify the defects in midwifery care and to establish applicable adjustment. Items
with positive clients’ perception need to be sustained and improved by midwives. Finally, this study may be
the first in its kind in midwifery so it will be a stepping stone for other researchers to do further studies in
the discipline of midwifery in Ethiopia and beyond.
The results have substantial importance to the service administrators in searching for ways to improve service quality by accommodating what antenatal care clients consider important with regard to acceptable caring behavior. Regardless of clients’ written reports, uncaring behavior must be further investigated and managed as a matter of determination. There is a need to conduct a large scale professional caring behavior assessment for the midwives to identify the measurable gaps. There is a need to conduct more broader research with midwives to gain more understanding of the link between support, burnout and staff turnover. Midwifery training should include and underline the emotional aspect of caring in the curriculum and assess caring behavior. Further studies that use CAT are recommended to understand mothers’ perceptions of the service they receive from midwives.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!