Biography
Interests
Bamidele Johnson Alegbeleye
Department of Surgery, St Elizabeth Catholic General Hospital, Shisong, Northwestern Region, Cameroon
*Correspondence to: Dr. Bamidele Johnson Alegbeleye, Department of Surgery, St Elizabeth Catholic General Hospital, Shisong, Northwestern Region, Cameroon.
Copyright © 2019 Dr. Bamidele Johnson Alegbeleye. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Acute mechanical intestinal obstruction is one of the leading causes of surgical admissions in
most emergency departments worldwide. The causes of intestinal obstruction vary significantly
depending on geographical location. The outcome of management of the condition may be a good
indicator of how well a country’s surgical services are doing. The aim of this study was to identify
the etiology, management and outcomes of patients with acute mechanical intestinal obstruction
presenting in rural mission hospital, North-western Cameroon.
This a retrospective descriptive study from January 2011 to December 2016. Data analyzed from
patients’ records included age, sex, duration of symptoms, operative diagnosis, treatment and
outcome of management.
There were 245patients with intestinal obstruction seen during the study under review. Males accounted
for 62% of cases. The ages of patients ranged from 2 days to 80 years with a mean of 38.9
± SD 11.9 year. The average duration of symptoms was 4 days. Acute abdominal pain, vomiting and
absolute constipation were the commonest symptoms. The leading cause of intestinal obstruction
was obstructed/strangulated external hernias found in 66 (27%) of patients and was followed by adhesions
with 54(22%) patients and the third being volvulus occurred in only 47(19%) patients. One
hundred and four (42%) patients underwent intestinal resection and anastomosis. The hospital stay
ranged between 1 and 36days with a mean stay of 10.4days. The overall mortality rate was 17 (8%).
Acute intestinal obstruction remains a serious health concern in our rural community. The high
rate of obstructed or strangulated hernias and the considerable morbidity as well mortality reflect
a poor health delivery system. This challenging situation can only be bettered by friendly environment
and improved health care facilities including active public health campaign for mass elective
hernia repair.
Introduction
Acute mechanical bowel obstruction is one of the commonest abdominal surgical emergencies globally with
considerable morbidity and mortality [1,2]. It constitutes a major financial burden in hospitals around the
world and a significant cause of admissions to emergency surgical departments [2,3]. Early diagnosis and
prompt management are therefore mandatory. Several factors contribute to poor outcomes in the case of
intestinal obstruction. Some of these determinants may include poor health seeking behavior, ignorance
and poverty. Poor clinical judgment is also one of the negative factors leading to poor prognosis in case of
intestinal obstruction [4,5].
In rural settings, Clinicians are more likely concerned about early recognition of intestinal strangulation in patients with mechanical bowel obstruction so as to decide on emergency surgery or to allow for safe nonoperative management of carefully selected patients [6,7]. The clinical picture, however of these patients [8-10] along with the etiology of obstruction [1,11-14] and strangulation prevalence are variable [7,15,16].
The pattern of intestinal obstruction is an indirect indicator of how well surgical services are developed in a certain region. Holcombe [17] compared the relative plethora of hernia and the paucity of adhesions to the high case mortality rate in Sierra Leone. In a related study, caeco-colic intussusception was the leading cause of intestinal obstruction in adult patients seen at Kibogora hospital [18]. Such a pattern of intestinal obstruction is seen in most of the countries which are not economically very prosperous. Interestingly, there is paucity of information about the spectrum of intestinal obstruction in our environment till date. This study was therefore undertaken in order to document the pattern of intestinal obstruction in St Elizabeth Catholic General Hospital, a rural mission Hospital in Northwestern region of Cameroon.
Patients and Methods
This was a retrospective descriptive study from January 2011 to December 2016. The study was conducted
at St Elizabeth Catholic General Hospital, a 250 beds missionary hospital in the Northwestern region of
Cameroon. The data retrieved from records of patients operated on for acute intestinal obstruction and
the following variables were collated including socio-demographics, duration of symptoms, preoperative
diagnosis, operative findings, procedure done, length of hospital stay and outcome. The results were analyzed
using SPSS version 21 for Windows.
Results
During the period under review a total of 268 patients were admitted with acute bowel obstruction. Twentythree
were excluded from the study due to incomplete records. The results presented are based on the
remaining 245 patients. There were 152 males (62%) and 93 females (38%), with a Male: Female ratio of
1.63:1.
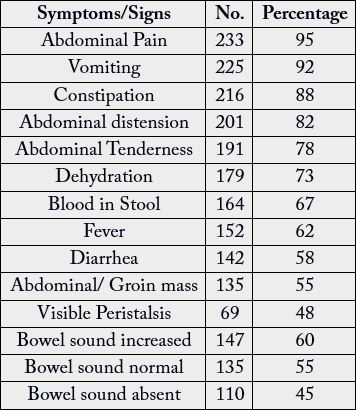
The ages of patients ranged from 2 days to 80 years with a mean of 38.9 ± SD 11.9 years. The duration of symptoms ranged from 1 to 14 days with a mean of 4 days. Only 90 patients presented within 24 hours after the onset of symptoms. Neonates and infants accounted for 8.6% of the patients. The majority of the patients (77.1%) came from rural areas. Acute abdominal pain, vomiting and absolute constipation were the commonest symptoms, while abdominal tenderness and abdominal distension were the leading signs. The hospital stay ranged between 1 and 36days with a mean stay of 10.4days. The overall mortality rate was 17 (8%)

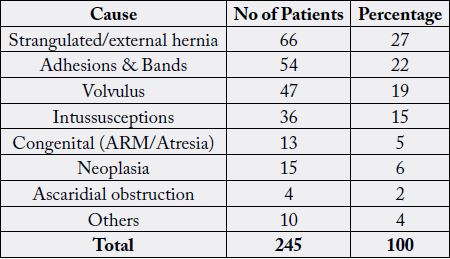
Based on Table 3 above the various causes of intestinal obstruction in St Elizabeth Catholic General Hospital, Northwestern, Cameroon were outlined. Strangulated external hernias were the commonest cause found in 66 (27%) patients. Indirect inguinal hernias were the commonest variety to strangulate in 36 (15%) cases, followed by para-umbilical hernia in 15(6%) cases, incisional hernia in 14 (6%) cases and femoral hernia in 13 (5%) cases.

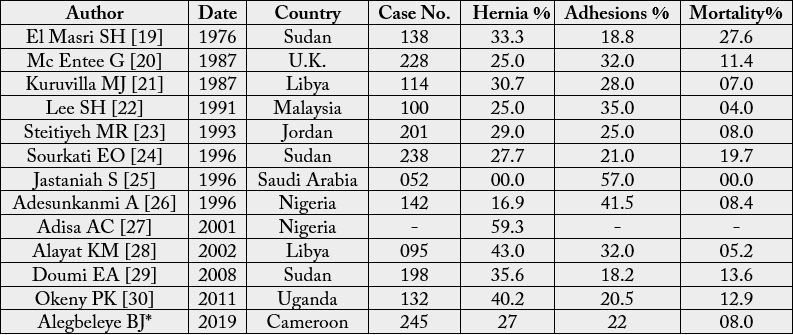
* The present study.
Discussion
This is a pilot study for the spectrum of causes of bowel obstruction and its management outcomes from
Northwestern region of Cameroon, where the society is changing fast and many factors like unfavorable
weather conditions, anglophone conflicts and displacement are prevalent.
Regarding clinical presentation of our patients, colicky abdominal pain, vomiting and absence of passage of flatus and/or feces were the most frequent presenting symptoms and abdominal distension was the most common physical finding on clinical examination as shown in figure1. Additionally, nausea, vomiting, colicky abdominal pain and abdominal discomfort were frequent symptoms on arrival. Our results, even though some differences are noticed, are in accordance with the literature [5,9,10,31]. Similarly, Cheadle et al reported abdominal pain (92%), vomiting (82%), abdominal tenderness (64%), and distention (59%) as the most frequent symptoms and signs [5,31]; whereas abdominal distension, bilious vomiting, absolute constipation and abdominal pain were the main signs and symptoms in another series [9, 31]. Perea et al prospectively studied 100 patients with adhesive small bowel obstruction and found that the presenting symptoms were vomiting (77%), colicky abdominal pain (68%), absence of passage of flatus and/or feces (52%), and constant pain (12%), whereas abdominal distension constituted the most frequent clinical sign with a prevalence of 56% [10,31].

In this study, males constituted 62% which is comparable to other studies [26,32-34]. Ntakiyiruta and Mukarugwiro [33] in their study reported a duration of symptoms of 3.5 days which is comparable with what we found but contrasted with Haridismos et al’s 33.5 hours [35]. Majority of the patients [60%] presented more than 24 hours after the onset of symptoms. This delay in presentation and/or surgical intervention frequently results in relatively poor surgical outcome and/or longer hospital stay [33,35]; which was evident in this study as shown in the statistics above. Reasons for delay may include poverty, long distance to care centers, scarce infrastructure and poor health seeking behavior [33, 36,37].
In this series, the four leading causes of obstruction included hernias, adhesions, volvulus and intussusception. Also 5% of the patient with congenital bowel obstruction; Figure 2 shows plain radiograph with doublebubble confirming duodenal atresia. Hernias are a leading cause of obstruction in most African centers [21,33,35,38] which may be caused by the paucity of surgical services in the region [17]. Hernias may occur in a congenital preformed sac (remains of processus vaginalis) or follow straining from heavy weight lifting, chronic cough, benign prostatic hyperplasia and urethral stricture or may follow a familial collagen disorder [37,39,40].

Strangulated hernias constituted 27% of cases and adhesive obstruction 22%. Similar figures were reported by Sourkati who reported strangulated hernias (27.7%) and adhesive obstruction (21%), from Khartoum [24,25,29]. This finding agreed with other reports from some developing countries [29,41-44]. A 57% adhesive obstruction and no strangulated hernia among 56 patients were reported in a district hospital from Saudi Arabia [28,29]. Such a high rate of adhesive obstruction was equally reported from the developed countries [29, 45], together with marked decrease of strangulated hernias, indicating that complications of hernia may be reduced with health education and elective hernia repair [29,45]. In other to achieve similar results as obtained in developed countries; our health delivery system must be welcoming and the service also user-friendly in style.
The types of strangulated hernias in this study were similar to the findings of Sourkati in Khartoum [24,29]. Indirect inguinal hernias were commonest to strangulated hernias followed by Para-umbilical hernias. The rate of bowel resection was 104 cases (42%), while the mortality rate was 17 (8%) of 245 cases studied. Another study confirmed this observation and found bowel resection was necessary in 37.5% of cases with 6.25% mortality rate [29,46], compared to bowel resection in 24.1% of cases and a mortality rate of 6.2% in Ghana [29,47]. Strangulation was described to be associated with up to 10-fold increase in intra and postoperative mortality [3,29].
Appendectomy, Caesarean section and abdominal trauma laparotomies were the commonest causes for adhesive intestinal obstruction. The reason is probably because those operations were performed as emergences at incontinent times by the junior staff. Although a conservative approach was globally adopted for the treatment of adhesive intestinal obstruction, but symptoms like continuous abdominal pain and fever; signs of toxemia, tachycardia, rebound tenderness, rigidity and absent bowel sounds may indicate the development of critical ischemia and/or gangrene.
Acute sigmoid volvulus was found in 47 patients (19%). The clinical features and management outcomes of the condition in this community were discussed previously [29,48]. Intestinal obstruction due to peritonitis occurred in 28 patients (11%). Intra-abdominal sepsis mainly resulted in patients with perforated appendix or typhoid ulcers [29,49]. Neoplasms, either of large or small gut are still an uncommon cause of bowel obstruction in many African centers [44,45,49] accounting for 15 cases (6%) mainly at the recto sigmoid with late presentation, while intussusceptions resulted in 36 cases of bowel obstruction (15%). The clinical presentations of acute intussusceptions in this society were outlined elsewhere [29,50]. Ascaridial obstruction was also found as an etiology of bowel obstruction in our study especially in four pediatric cases. This was similar to a study done in Kashmir by Shiekh KA et al [51] where ascaridial obstruction was the commonest etiology. This observations are also in variance with other Indian series [20,51-56]. Poor hygiene, improper sanitation and waste disposal encourage the multiplication of Ascaris Lumbricoides in places like our setting.
Strangulated obstruction requires emergency surgery, and early recognition is often life-saving since delay in treatment is an independent predictive factor of mortality and, in addition, bowel strangulation is an independent predictor of complication and, even more, of mortality while the mortality rates of patients with strangulated obstruction are two to 10 times higher than those of patients with non-strangulated obstruction [31,57,58]. Moreover, accurate early recognition of intestinal strangulation in patients with mechanical bowel obstruction is important to allow safe non-operative management of carefully selected patients [1,2,6,7,31].
Traditionally, such recognition is based on the presence of one or more of the classical signs: vascular compromise, continuous abdominal pain, fever, tachycardia, peritoneal signs on physical examination, leukocytosis, and metabolic acidosis [6,7,31]. Close and careful clinical evaluation, in conjunction with laboratory and radiologic studies, is essential for the decision of proper management of patients with acute mechanical bowel obstruction; if any uncertainty exists, prompt operative intervention is indicated [1]. It should be emphasized, though, that great caution should be taken for the management of these patients since studies have shown that preoperative diagnosis of bowel strangulation cannot be made or excluded reliably by any known clinical, laboratory, or radiologic parameter, combinations of parameters, or by experienced clinical judgment [6-8,31].
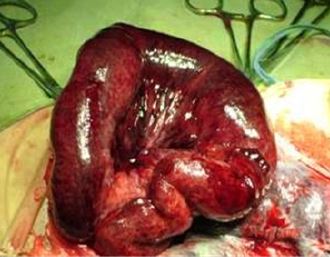
In this study; 104 patients (43%) had gangrenous bowel at operation (Figure 3,4 and 5), for which resections and anastomoses were done (Figure 3,4 and 5). In a similar society 32.4% of patients with gangrenous gut needed immediate resection and the procedures resulted in a mortality of 17.3% [29,59]. Recently in a developed community it was reported that ischemia, necrosis and perforations accounted collectively for 28.6% of patients with bowel obstruction [29,31].


Data regarding management and outcome of the patients as described above showed that One hundred and twenty-nine patients (52.5%) of the total study group were safely and effectively treated conservatively. In seven patients resuscitation failed and they died before surgical intervention, all of them were at the extremities of age i.e. neonates, infants and elderly. Ten patients died after surgery. Out of these three were elderly males who developed pneumonia, two were infants with generalized peritonitis and the rest (14 cases) were found to have had gangrenous bowels for which resections and anastomoses were done, accounting for almost 10% of bowel resections. In a similar setting Ohene-Yeboah et al reported a mortality of 12% in patients who underwent emergency bowel resections due to ischemia [29,39]. The most probable causes of death were electrolyte imbalance and septic shock. Postoperative morbidity was mainly wound infection with prolonged hospital stay. Two patients had burst abdomen and another patient developed an incisional hernia.
Conclusion
Acute intestinal obstruction is a serious surgical emergency. Strangulated external hernias, adhesions and
volvulus were the leading causes, similar to patterns reported many decades ago from elsewhere. Less common
causes were peritonitis, large bowel tumors and intussusceptions. The high rate of strangulated hernias and
the considerable morbidity and mortality reflected a poor health delivery system. This challenging situation
can only be bettered by friendly environment and improved health care facilities including active public
healthcare plans for mass elective hernia repair.
Declarations
Not Applicable.
No record of funding for this Clinical Research Study declared
All data generated or analyzed during this study are available for review by the Editor-in-Chief of this
journal.
The author has no disclosures.
The Author conceived of the study and participated in its design and coordination and helped to draft the
manuscript; Also read and approved the final manuscript.
Institutional Ethical Approval was granted for this study and available for review by the Editor-in-Chief of
this journal.
This is a retrospective descriptive study; therefore there is no direct human participant’s involvement.
There is no submission of any financial and non-financial conflict of interest.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!