Biography
Interests
Mila Bunijevac1*, Mirjana Petrović-Lazić2,3 & Siniša Maksimović1
1Public Health Hospital “Sveti Vrači”, Bijeljina, Bosnia and Herzegovina
2Faculty for Special Education and Rehabilitation, University of Belgrade, Serbia
3ENT Clinic, Clinical Hospital Center “Zvezdara”, Belgrade, Serbija
*Correspondence to: Dr. Mila Bunijevac, JZU Hospital “Sveti Vrači”, Srpske Vojske 53, Republic of Srpska, Bosnia and Herzegovina.
Copyright © 2019 Dr. Mila Bunijevac, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
The aim of the study is to carry out a subjective assessment of the voice in patients with hyperkinetic
dysphonia before and after vocal rehab.
In this study, 20 subjects with hyperkinetic dysphonia participated. A subjective voice assessment
was conducted using the Voice Handicap Index - VHI instrument, which includes three aspects:
functional, emotional and physical. This instrument can provide information on the stage of the voice problem experienced by the patient himself and the impact of vocal rehabilitation before and
after treatment.
Prior to vocal rehabilitation, heavy vocal disorder was prevalent among the respondents, which
had a negative impact on their professional, social and emotional functioning, and after vocal
rehabilitation there was an improvement in the voice of all respondents.
Vocal rehabilitation has given positive results in this study in subjects with hyperkinetic dysphonia.
Introduction
Hyperkinetic dysphonia is the most common voice disorder, both in adults and children. It is characterized by excessive use of muscle power at the level of the generator, activator and voice cutter. If such a voice disorder lasts for a long time, it can get to the settled wrong one automation of phonation, which is difficult to correct, and in some cases it is impossible to correct them [1].
Hyperkinetic dysphonia is most often encountered by vocal professionals, such as lecturers, sports coaches, street vendors, command staff, and so on. They speak a little louder, which for the octave is more than the basic normal voice, they invest a lot of effort on the generator and damage its function. This condition is especially characteristic for children. It is reported in children of both sexes who have a striking desire for domination in the group [2,3].
Risk factors for the development of hyperkinetic dysphonia are inflammatory processes, occasional hormone imbalance leading to certain changes in larynx, genetic and neurovegetative factors, speech in the noise, when patients have to overcome the surrounding noise level [4].
Hyperkinesia at the level of the voice generator can be due to hard voice voices, the use of inadequate voice, voice abuse, and laryngeal support. Hyperkinesia at the level of the voice activator can be due to a high type of breathing, taking excessive amounts of air during phonation, short breath and low intensity function. Hyperkinesia at the level of voice resonance can be due to phonation with excessively tense pharynx walls, wrong position of tongue, soft palate, and small or excessive opening of the mouth.
Symptoms of hyperkinetic dysphonia can be divided into subjective and acoustic. Subjective discomforts are discomfort and throat dryness, sometimes throat and neck pain, tiredness of the voice and mischief of varying degrees. Acoustic symptoms of patients with hyperkinetic dysphonia are manifested by a weaker or stronger tummy, a voice is tightened, a reduced volume, and a hard start of fonation. If the patient uses a voice like this for an extended period of time, an aphonia may occur [5].
The diagnosis of these patients involves: laryngoscope, video stroboscopic examination, radiological examination, electromyographic examination, computerized voice analysis (objective assessment) and subjective voice assessment.
Phoniatric rehabilitation includes in addition to medication therapy and vocal rehabilitation. Vocal rehabilitation is focused on mastering the technique of proper breathing, removing tension in the neck and shoulder belt, providing and guiding vocal hygiene guidelines [6].
The aim of the study is to carry out a subjective assessment of the voice in patients with hyperkinetic dysphonia before and after vocal rehab.
Materials and Methods
The present study was carried out to evaluate the sensitivity pattern of Cefaclor and Cefixime against 100
isolates of Staphylococcus aureus and Escherichia coli. for this purpose clinical isolates was determined by disc
diffusion method.
In this study, 20 patients with diagnosed hyperkinetic dysphonia participated. The research was conducted
at the JZU Hospital “Sveti Vračevi” in Bijeljina. All respondents were first examined by a specialist in
otorhinolaryngology, by methods of indirect laryngoscopy and videostroboscopy, after which they were sent
to the logopedic clinic where vocal rehabilitation was conducted twice a week for 30-40 minutes.
In this study, a subjective voice assessment was performed using the Likert-type instrument, the Voice
Handicap Index (VHI) [7], which includes three aspects: functional, emotional and physical. Each aspect
contains 10 questions - five choices (0-4). This instrument can provide information about the degree of voice
problem experienced by the patient himself and the impact of vocal rehabilitation before and after treatment.
Patients completed the questionnaire twice, the first time before the start of treatment and the second time
after its completion. Question completion time was not limited. Each respondent was an explicit research
draft.
Statistical data processing used descriptive measures, arithmetic mean with the corresponding standard
deviation as well as minimum and maximum. Frequency and frequency were used precedents. Statistical
processing and analysis was done in the computer program SPSS ver. 20 (Statistical Package for the Social
Sciences).
Results
In this study, 20 respondents, 13 female and 7 male respondents participated. (Table 1).
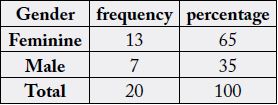
f - frequency; % - percentage
The age of the subjects ranged from 23 to 56 years, the average age of the respondents was 40.05 years. Treatment length ranged from one to two months (Table 2).

N - number of respondents; Min. - minimum; Max - maximum; M - arithmetic mean; SD - standard devation
The Voice Handicap Index (VHI) scale was used to evaluate the psychosocial functioning of patients before and after vocal rehabilitation. The patients filled out the questionnaire with their opinion on the voice problem, their difficulties, or the smaller or larger restrictions that created their voice in personal and professional life.
The analysis of subjective voice evaluation before vocal rehabilitation indicates a severe physical disorder in all respondents (100%). On an emotional syringe, 70% of the subjects had a severe, 20% moderate and 10% mild voice disorder. On functional supplements before treatment, there is no mild voice disorder, 30% of respondents have moderate and 70% have severe headache (Table 3). Based on the analyzed parameters, the respondents expressed already bio-psycho-social difficulties in their voice quality, which had a negative impact on their professional and social functioning, as well as their emotional state.
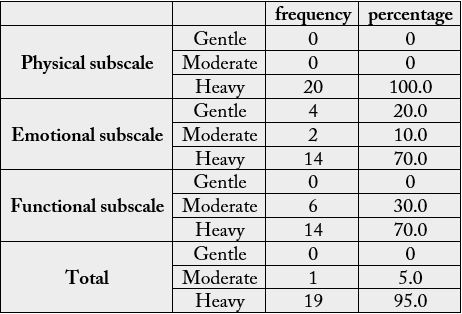
f - frequency; % - percentage
After vocal rehabilitation, all respondents (100%) on all the supplements had mild voice problems, which did not affect any aspect of their life (Table 4).
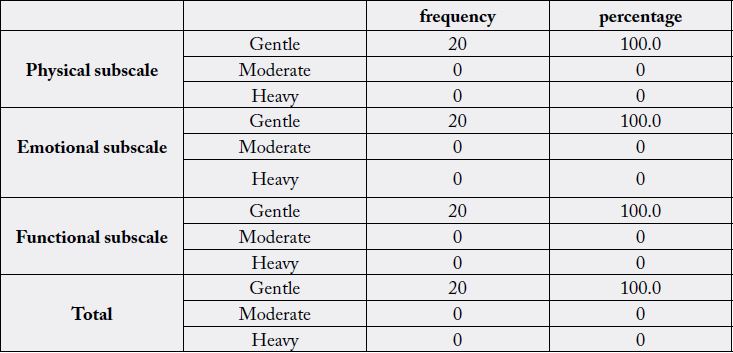
f - frequency; % - percentage
Discussions
Hyperkinetic dysphonia is most often caused by the wrong use of the vocal apparatus. It causes a variety of
different intensities that can negatively affect the physical, emotional and social aspects of life.
In this study, female respondents were mostly female. The average age of the respondents is 40.05. Results in this study are comparable with the results of other studies [8].
The duration of treatment ranged from one to two months, on average patients had eight to ten treatments.
The results obtained before vocal rehabilitation indicate a severe physical disorder in all subjects. These results are consistent with previous studies where it has been confirmed that dysphonia can cause emotional difficulties that negatively affect the patient’s social functioning [9-11].
After vocal rehabilitation, all the respondents achieved complete improvement in their voice, which means that vocal rehabilitation gave positive results. Many studies have shown that vocal therapy can lead to improved voice quality [12-15].
Vocal rehabilitation eliminates the unnecessary tension of the larynx and neck muscles, allowing the proper flow of air current [16,11], with the implementation of vocal hygiene measures [15].
Conclusion
Hyperkinetic dysphonia can negatively affect the quality of life of patients. However, by vocal rehabilitation,
patients can correct their voice problems, which positively reflects primarily on their emotional state and,
consequently, on their working and social functioning.
Conflict of Interest
The authors state that there are conflicts of interest in relation to this article.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!