Biography
Interests
Sukant Garg*, Sajal Afzal & Jagdish Chandra Garg
Garg Nursing Home, Mahadji Park, Gwalior, Madhya Pradesh, India
*Correspondence to: Dr. Sukant Garg, Garg Nursing Home, Mahadji Park, Gwalior, Madhya Pradesh, India.
Copyright © 2018 Dr. Sukant Garg, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Adolescents are at risk to contract a majority of sexually transmitted diseases (STDs). On a usual note, adequate knowledge about sex has been missing in them due to the relatively limited exposure to the literature, which hampers their decision-making capacity. As a result, they have shown a high incidence of STDs in the recent years. Topics covered under sexual education are often ignored or misunderstood due to inappropriate curriculum and taboos with socio-cultural reasoning. The target of this report is to identify the reasons for these failures and to introduce a strategy to undo them. Our highlight is the obligation of certain measures to ensure the extraction of valuable output. Purpose of sexual education should be to provide information on ‘sexuality’, ethics, abuse, complications and general therapeutic management. Implementation of sexual education in younger years of life could be beneficial; it should be planned based on age and intellectual capacity of audience, and executed according to the language and region. Joint involvement of family, friends and teachers could be more productive. Social leaders should be positive involved. Government and non-government organizations should co-operate for unbiased implementation.
Introduction
Adolescence is the age ranging from 10 to 19 years, characterized by a series of mental and physical changes.
Adolescents acquire independent thoughts gradually and engage in love, relationships and sexual contacts.
They are at risk to a majority of sexually transmitted diseases (STDs) [1]. On a usual note, adequate knowledge
about sex has been missing in this age group due to the relatively limited exposure to the literature and wisdom.
As a result, they have shown a high incidence of STDs in the recent years. Adolescence is the age when
one best learns and adapts their lifestyle owing to the education earned. Some of the commonest forms of
STDs are chlamydia, gonorrhea, herpes, syphilis, and Human Immunodeficiency Virus/Acquired Immune
Deficiency Syndrome (HIV/AIDS) [2]. Chlamydia is known to be most common in late adolescence in
men and early in women; syphilis is usually common in young women and middle aged men; gonorrhea
contracted more hundreds of thousand cases in 2009 according to the Centers for Disease Control datasheet;
Herpes Simplex Virus infected about a sixth of working young Americans population in the recent years;
Human Papilloma Virus has more than 40 different schemes to infect; HIV/AIDS infection has been
butchering living beings to death since decades. These infections are found to be more in people practicing
unhealthy sex, unprotected sex or homosexuality and abusing. In men, when one is sexually aroused, the
brain sends nerve signals to penile tissue and causes tissue expansion, hardening and blood pooling in penile
sinusoids. Interruption in the process causes impotence or erectile dysfunction [3]. It can lead to low selfesteem,
poor sex life, relationship disturbances, stress, depression and failure to settle. Use of condoms could
control the rate of this to a significant magnitude [4].
Many young sexually active women fail to understand that practicing oral contraception methods may not
always be adequate, and is probable to failure [5]. This has resulted into many false conceptions, complications
of termination, and STDs - among the teenagers! Todays’ college going students form the most vulnerable
and risky population as they lack adequate knowledge about sex, and practice behaviors like unprotected sex
and substance abuse. People believe that oral sex is risk free [6]. Many fantasize rape as pleasure. Accidents
while these may lead to deadly outcomes such as STDs. Nearly 5-10% of pregnancies reported globally
are accidental [7]. Not rarely the patients haven’t even heard of medical termination of pregnancy (MTP).
Those who know mostly decide to terminate and end up picking up life-threatening complications. Few
steps that can help reduce MTP-related morbidities to a great extent are expanding access to health care
system, training healthcare personnel, maintaining supplies and equipment at the first referral facility, and
most importantly a high regard to ethical guidelines. There is a need of youth friendly programs such as
condom promotion and volunteering. Research has shown that condom promotion programs have managed
to encourage sexually active youngsters to use condom and thereby reduce risks of STD transmission and
accidental pregnancy. In a cost analysis, it was found that medical expenditure spent to manage STDs was
significantly higher than the cost to organize these campaigns. Hogg et al. screened over 90000 patients and
22 intervention primary care practices to conclude with about 40% health-cost benefits [(improvement in
health + reduction in medical care cost)-(program methods + materials)] [8,9].
Reports about the barbaric practice of female genital mutilation (FGM) cautioned readers about its rampancy in some of the most powerful nations such as the United States of America, Australia, Germany and India [10-12]. FGM is a ritual removal of whole or part of external female genitalia, with or without the use of local anaesthetics. It is considered analogous to circumcision in males. Believers in this brutal practice allude gender inequality, controlling women’s sexuality, purity, modesty and beauty to reasoning. The World Health Organization and many other organizations for about a decade have been taking extensive initiatives to completely abolish it, but only trivial progress has been made (Organization 2018) [13]. Despite of strict laws and opposing factors, FGM is finding its way into the actuality [14]. We believe that a frank lack of education about sexuality could be the reason behind the swelling global index of FGM.
Numerous sex-kindred scandals such as rapes, female feticides, drug abuse and gender-based favouritism are reported every day that create demoralizing site for social development and lead to civil anarchy. Creative ideas, proactive attempts and frank discussions are required to improve sexual relationships, and to attract youngsters to participate. These days, even if a youngster is willing to learn on the topic, she/he has to refer to many indirect, informal and unethical sources. Direct resources such as a licensed practitioner or printed journals are either expensive or out of bound. Growing ‘sexuality’ in media these days is deceiving the juvenile intellect by advertising sexuality irresponsibly. There are few initiatives taken around the world to combat these problems. We read about the abstinence-only programs implemented by various institutions, where the students are trained and encouraged to abstain from sex before marriage [15]. Reports say that such programs educate the students about the reproductive health and birth control, but it does not teach safe sex, or prevent unsolicited pregnancy or STDs. Furthermore, their alumni often show unwillingness to use healthy contraceptive methods when most required [16,17]. Abstinence-only programs violate fundamental human rights, such as right to information and freedom [18,19]. We have tried to identify the reasons for the failure of these programs to positively impact the society, and to suggest measures to rectify them.
Sexual education (SE) is the realization of one’s sexuality, in an ethical and guided manner. SE begins right
at birth (for example, joy felt by a baby to the physical contact by the mother), and continues throughout
life. It is an integral part of one’s physical, mental and social development. It provides information and values
related to one’s sexuality, not only to live one’s own life, but also to maintain healthy relationships and
fulfil social responsibility to others’ sexual well-being. It helps to explore a person’s values, and develop attitude
and communication aiming to reduction of sex-related risks and overall decision-making. SE is not
just education about human reproductive biology and STDs as traditionally mentioned. We believe that
the SE is age-dependent, culture-relevant, unbiased, realistic, straight-forward information about a person’s
sexuality, including physiological and pathological aspects. Topics covered under SE are often ignored or
misunderstood due to inappropriate curriculum and taboos built up with socio-cultural reasoning [20]. Our
focus is on the effective implementation of SE. Its purpose should be to provide information on ‘sexuality’,
ethics, abuse, complications and general therapeutic management.
Schooling is common to all children and it bears the age the when a child first discovers her/his sexuality, therefore quite naturally, it is the most suited platform to teach about the most misunderstood and tabooed topic. Parents and teachers are primary SE providers [21]. They are the first people to whom a child turns to ask some of the most intimate questions about herself/himself. Any form of misguidance at this time may prove to be catastrophic in their later lives. Other meaningful resources to acquire information include books, electronic media (such as eBook, articles, CDs and educational websites), health care providers, teachers, and campaigns programmed to deliver SE. SE contributes meaningful inputs to five out of the eight Millennium Development Goals set by the United Nations (UN) (universal primary education; gender equality and women empowerment; child mortality; maternal health; combat against HIV/AIDS, etc.).
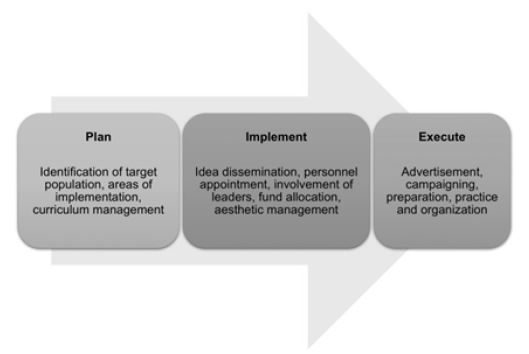
One of the important goals of SE is to ensure development of equitable interpersonal relationships [22]. Studies suggest that the education rank is directly proportional to the behavioral responsibility by a person [23]. In 2014, a systematic review and meta-analyses on sexual knowledge and responsive behavior in lowand middle-income countries showed positive behavioral changes (delayed sexual debut, decreased number of partners and increased condom use) in school children [24]. Hence, implementation of SE in younger years of life is important; it should be planned based on age and intellectual capacity of audience; it should be executed according to the language and geographical region. Involvement of the children along with their peer, parents and teachers could be more productive. Social leaders should be positive involved. Government and non-government organizations should co-operate for unbiased implementation. Short-term benefits of SE may be intercourse debut delay, reduction in teenage sex, sexual partners and unprotected intercourse, use of condoms, and awareness. While the long-term may include reduction in the incidence of STDs and unwanted pregnancies, improved nutritional and mental health, and population control. Effective implementation of SE could help accustom the mind-set of beneficiaries to practice it.
Campaigning a SE program is not easy. It is difficult to pilot a campaign and program it to national/global
level and to maintain its progress [25]. It requires financial and political support, and a smooth trajectory so
that the basic essence of individual attention does not get away. The most significant restricting factors to SE
programs are political (fear of losing votes), religious (overdependence on faith), parents (communication
gaps), professional (ethical boundaries and lack of motivation) and financial (lack of funds). Unites States,
Mexico and Kenya have faced strong opposition by religious groups against school-based SE [26,27].
Conservative forces in India have hurdled SE in schools. However, despite strong challenges and critics,
few countries like Egypt, Mali, Pakistan, and Yemen have yet managed to successfully implemented such
constructive programs. It is difficult to disseminate information on such wide scale, yet many significant
achievements have been made. In 1989, UN held Convention on the Rights of the Child, which conceived and
acknowledged the rights of a child to information [28]. Right to knowledge, is indeed necessary for effective
implementation of SE. Sweden was the first country to implement SE as a mandatory subject officially in
1955 [29]. It was then followed by Germany (1968), Austria (1970) and later Netherlands and Switzerland.
In Ireland, it has been mandatory since 2003 despite of the strong religious opposition. Government of
these countries soon recorded a sharp prune in sex-related morbidities post SE implementation. Global
organizations such as UNFPA, UNESCO and UNICEF have been organizing programs to promote SE
[30-32]. World Bank is one of the premier institutes to have been continually challenging STD progression.
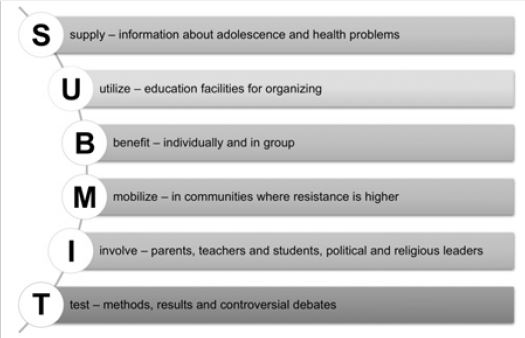
In order to overcome the opposing factors to SE, we suggest the strategy SUBMIT (supply: information about adolescence and health problems; utilize: education facilities for organizing; benefit: individually and in group; mobilize: in communities where resistance is higher; involve: parents, teachers and students, political and religious leaders; and test: methods, results and controversial debates). Since SE had been a soft target for misunderstandings, it should be conducted based on set principles: it must be age-appropriate, directly related to the life of the student, aimed to improve health, accurate and based on scientifically proven facts, within ethically boundaries, by a well-trained and motivated staff, interactive and motivating, should promote counseling, should teach the importance to respect sexuality, should discourage violent behavior, should encourage students to research, and should answer critics with continual feedback. Here are a few additional constructive measures - officially implementing a definite course and open-minded delivery, bringing specialists to talk about the sexual health related topics, conducting basic level examination based on pre-defined syllabus, encouraging co-curricular activities concerned with SE, counselling at each health check-up, setting up campaigns and promotional advertisements, and actively involving experts and leaders to promote and give value to the cause. In all, we believe that it is important to formally mandate implementation of SE across the world in a region-specific manner. However, the ground concepts and principles must be the same. Sexual Education has potential to tremendously prevent the future social contaminants.
Conclusion
Adolescence is the most common and unhealthy at risk age group to acquire sexually transmitted diseases.
It’s the age when a person can best learn and adapt to long-lasting lifestyle by means of the education and
information they attain. Topics Covered under sexual education i.e., sexually transmitted diseases, impotency,
unintended pregnancy and abortion, are often left out or misunderstood due to faulty educational faculties.
Various social taboos, and associated socio-cultural and religious issues pose a serious threat in the path
to escape this crisis. Education is directly related to the social-behavior, is age-dependent; therefore, the
measures must be set universally as well as individually. Positive Involvement of the teachers, family, and
political and religious leaders would help greatly, so will the regional approach, linguistic basis, and sociocultural
respect. The purpose of sexual education is to provide information and promote awareness related
to diseases, treatments and means of infection. It would also create jobs and encourage inter-personal
relationships. Mandatory Sexual Education is the key concept that, when applied in the right manner and
time can tremendously and effectively improve the living conditions in the society. A thorough knowledge
about the topic should bring about all those starved changes to the world, like reduction of sexually
transmitted diseases, sexual respect of one person by another and peace and satisfaction in one’s mind as far
as love, relationships and sexual contacts are concerned. Based on the information gathered and studied, it is
clear that the society is waking up against the alarms and threats that the sexually transmitted diseases, and
other sex related medical/ethical issues sound. But however, in billions of populations, it is hard to maintain
the optimum levels of literacy and sense if it left on its own. Therefore, it is crucially important to make the
sexual education mandatory worldwide under the name of law. Sexual education officially must be started
not later than the onset of appearances of sexual characteristics (7th-8th grade), as it is the time where a child/
teen favors his/her thinking according to what the sexual hormones and personal ethics suggest. As it is
a highly controversial area and a huge area for debate, it’s learning must not stop until the person is fully
matured mentally and has a balanced sense of ethical awareness.
Notes
1. School going students have been shown better knowledge based feedback and prognosis for education
than any other age-groups.
2. Sexual education invites long-term benefits and effects health of the working population directly.
3. Various international banks and not for profit organizations participate actively to support and promote
initiatives such as sexual education.
4. Such an initiative has the potential to bring the society including leaders together on the same front.
- Dissemination of age-specific, realistic, graphical, accurate, scientifically challengeable and ethical
information,
- Must be handled sensitively by highly-motivated, trained and open-minded professionals, on a regular
basis, on an individual basis,
- Must be unbiased (sexual orientation, gender, ethnicity),
- Aims to develop fundamental skills (communication, negotiation, self-realization and reflection, decisionmaking,
problem solving),
- Must involve family members, teachers and group leaders,
- Encourage further research and diversification.
- Implementation and early initiation; mandatory, friendly, with examinations; definition of course and
contents, systematic study,
- Interactive approach in teaching, additional extra-curricular activities; peer activities; bringing specialists
to talk,
- Regular health check-ups, developmental training; professional scope and opportunities; campaigns and
promotional advertisements; youth-friendly services, social marketing of condoms,
- Involvement of religious leaders and influential identities; ethical and legal boundaries.
- Reduction in frequency of unsafe teen sex
- Increased awareness and hygiene maintenance
- Reduction in the number of sexual partners
- Reduction in the rate of acquiring sexually transmitted diseases
- Reduction in the number of unwanted pregnancies
- Ethical involvement and promotion of respect of women
- Reduction in the number of child marriages
- Improved nutritional status and overall health of the youth
- Improved mental healthy
Acknowledgements
Authors would like to thank emeritus professor Mr. Richard Booth from the Aston university for his valuable
guidance.
Disclosure Statement
Authors declare no potential conflicts of interest
Funding
Not applicable
Data Availability Statement
Not applicable
Data Deposition
Not applicable
Supplemental Online Material
Not available
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!