Biography
Interests
Pavel Sidorov, I.
Institute of Mental Medicine, Northern State Medical University, Arkhangelsk, Russia
*Correspondence to: Dr. Pavel Sidorov, I., Institute of Mental Medicine, Northern State Medical University, Arkhangelsk, Russia.
Copyright © 2018 Dr. Pavel Sidorov, I. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
The established feature of the modern world is a steady growth on the prevalence of all the major psychiatric disorders. The global predictor of this trend is the psychic traumatization of childhood and chronic psychosocial stress, triggering cumulative mechanisms of neuroepigenetic and epidemic development of mental immunodeficiency.
The task of the study is to describe the dynamics of the syndrome of mental immunodeficiency (SMID) in the early psychic traumatization of children. Mental immunity (MI) is a multimodal interface of consciousness and biopsychosociospiritual identity matrix as the basis for the security of the individual and society. The pathogenetic basis of the SMID is epigenetic accumulation in many generations of functional (reversible and dynamic) MI disorders that predetermine the change in the level and quality of mental health.
In the development of an epigenetic pandemic of traumatogenic mental immunodeficiency, six fractals are identified: 1) traumatogenic family; 2) pre-traumatic diathesis; 3) acute psychic trauma; 4) full-scale clinical picture; 5) chronization; 6) outcome. The main clinical manifestations of MI dysfunctions as a multimodal interface between identity and consciousness of an individual and habitat are described and systematized. Thus, the “missing link” between epigenetic pathogenesis and clinical pathoplasty of mental disorders is found. Multidisciplinary preventive-corrective and treatment-rehabilitation protocols and programs on the technological platform of mental medicine are proposed. The expression of Nobel laureate Peter Medawar, which became a textbook: “Genetics proposes, epigenetics disposes”, is appropriate to be supplemented by the mission of mental medicine, which embodies and implements project models of quality and style, the image and meaning of life in the adaptive neuroengineering and self-management of consciousness and health.
Introduction
The feature of the modern world is a steady increase in the prevalence of all major mental and psychosomatic
disorders. The global predictor of this trend is in many ways the psychic traumatization of childhood and chronic
existential stress. They trigger transgenerational and cumulative mechanisms of epigenetic development of
the pandemic of mental immunodeficiency (PMID). The task of the study is to describe and systematize
epigenetic dysfunctions of MI, clinically manifested by the SMID and triggering epidemiological cascade:
mental epidemic - destructive mental epidemic - pandemic of mental immunodeficiency. Early stress has
both acute and long-term effects on epigenetic labels in the brain, which are the interface of MI, affecting
cognitive functions and behavior, the risk of suicide and injurious acts or civil wrongdoing, dependent and
psychic disorders throughout the life of today’s and tomorrow’s generations. SMID is clinically represented
by a variety of borderline identity disorders. The pathogenetic basis of the SMID is the epigenetic
accumulation of functional (reversible and dynamic) disturbances in the MI as a multimodal interface of
consciousness and a biopsychosociospiritual identity matrix and the basis of security of the individual and
society. The MI is in many respects a standard placeholder, denoting the missing or indeterminate parameter
or operator in the network of the relationship between identity and behavior genome and epigenome.
Functional family diagnostics and screening in mental medicine (MM) make it possible to focus clinical
research on the entire accessible generational line: great-grandchildren - grandchildren - children - parents -
grandparents - great-grandparents. This makes it possible to assess and predict latent genetic and epigenetic
predictors by calculating probabilistic scenarios and trajectories of development of destinies. Our long-term
studies of the early psychic traumatization of childhood have shown the multivariance of changes in MI
and biopsychosociospiritual characteristics of the “traumatogenic family”, depending on the severity and
duration of transgenerational stress burden. The clinical features of new generations of the “traumatogenic
epigenome” depended significantly on external conditions: the same behavioral models (which are constant
for humanity) gave completely opposite effects in different social environments. That is why only the
synergetic biopsychosociospiritual methodology of MM allows designing effective integrative programs for
the protection of public health.
Synergetic Biopsychosociospiritual Methodology of Mental Medicine
Synergetics is a multidisciplinary science about the development and self-organization of complex dynamic
systems (including psychopathology development), the main functional principles of which are: nonlinearity,
non-stability, openness, dynamical hierarchy, observability. The methodology of synergetics is based
on the integrative approach to the study of structures which are thermodynamically open, non-equilibrious,
exchanging energy, information and substance with the environment of dissipative structures.
Dissipative structures are discrete self-organizing systems dissipating energy and distinguished by their spiral formation in multidimensional space, which trajectory and self-vibrating amplitude have a multivariant nature and are predetermined by a combination of differently directed forces and factors in bifurcation points. Dissipative structures exist and are formed in the society and the biosphere and intermittently go through self-organization processes following their internal development logic, becoming more complicated or degrading throughout their existence.
In synergetics, an important concept is a strange attractor. It is an object in the phase space that almost all trajectories aim for and upon which they are unstable. Attractors are classified as fractals (Latin fractus - fragmented) - objects characterized by their fractional size and multidirectionality of developmental trajectories. A fractal is a self-similar figure made up of parts that are each similar to the whole figure and have an uncommon structure. For example, fractal architecture and design are repeated at micro-, meso- and macro levels from DNA molecules to galactic spirals. In clinical medicine, a fractal is both development and state uniting time and qualitative characteristics of systems or bodies. A fractal is a projection on the scientific field of quantum concepts.
Fractal dynamics is a transition of a quantum system from one possible state to another via bifurcation, having passed which, a dissipative structure starts aiming for a new attractor. In clinical medicine, it corresponds to the development of psychosomatic disorders or recovery - depending on which of the attractors (leading to progression or remission) turns out to be currently important.
It is impossible to imagine isolated human psychosomatic health without interactions and influences of many internal and external factors. As a result, complicated and non-linear, unstable and open self-organizing dissipative systems appear.
We have developed a synergetic biopsycho-sociospiritual conception of ontogenesis that is represented by a tetranuclear or four-dimensional model consisting of vectors or planes of somato- and psycho-, socio- and animogenesis (Figure 1) [1,2].
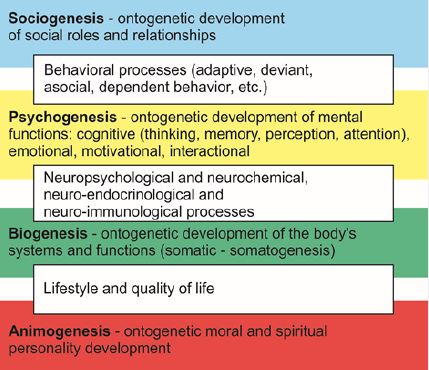
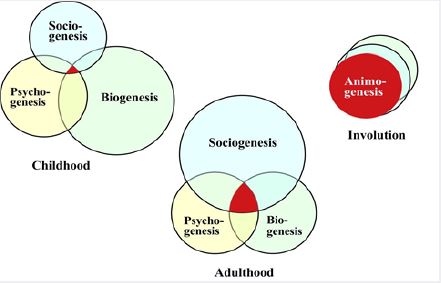
Anima, animus (Latin anima - soul, and animus - spirit) are concepts that in the Ancient Greek culture framed the phenomenon of spirit and acted as stages of the evolution of spirituality understanding: if anima (soul) is inseparable from its material carrier, then animus (spirit) has an autonomous status. Animogenesis is a term that integrates understanding of soul and spirit, specifies the central fourth part of the proposed ontogenetic model (Figure 2). The main ontogenesis planes interpenetrated and determined transit zones and a central part containing consciousness - the highest level of self-regulation and reflection of reality accumulating spiritual-moral potential.
The model presupposes a multidisciplinary and integral approach to complex and complicated psychosomatic cause-effect relationships. Trajectories of state or disease progress are determined and corrected at bifurcation points acquiring spiral-like properties and multivariance. For a better visual perception, Figure 3 presents a linear trajectory of psychosomatic diseases progress.
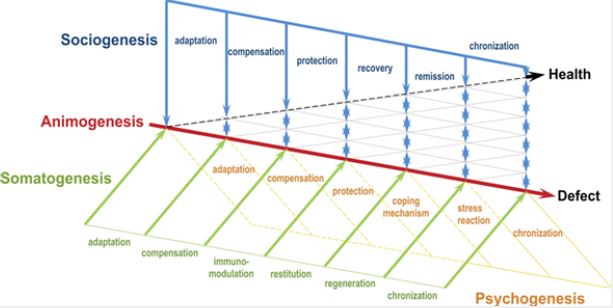
The traditional linear dynamics is changed by the synergetic non-linear fractality. Synergetics considers a human body as a complicated open system with non-linear processes. Such behavior is based on polymodal mechanisms of defense and appearance of internal fluctuations. After accumulation of a big number of fluctuations as risk factors echo, they produce cascade and cumulative effects at the bifurcation points changing the system development trajectory.
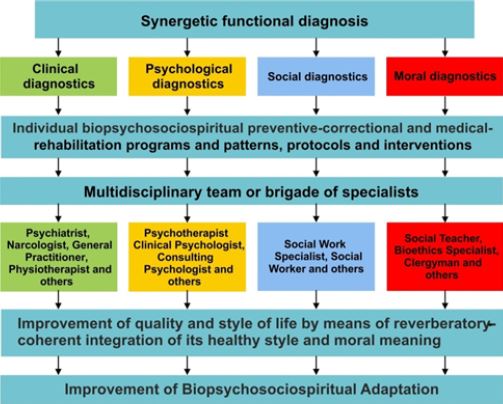
The proposed methodology makes it possible to formulate clinical and psychological, social and moral diagnoses taking shape of a syndromic synergetic functional diagnosis (Figure 4). Only such approach allows effectively carrying out personalized multidisciplinary protocols in mental medicine [1,2].
Etiopathogenesis of the Early Psychic Trauma
Clash of the child’s world with the world of adults, other children and a variety of events is not always
painless for the child. Sudden life events with a high degree of probability predispose to the occurrence
of child’s psychic disorders. If by their nature they are psycho-traumatic, they cause the long-term adverse
changes in life circumstances, lower the self-esteem.
Chronic stress, inevitable in any country in the transitional period has led to an increase in the incidence of psychogenic disorders, alcohol and drug abuse, increase in mental retardation. It is known that about 10% of all children have at least one parent who has serious psychic disorders. In recent years, there is a noticeable rise in the number of social orphans - the children, whose parents are deprived of parental rights. In Russia, there are more than half a million orphans, who are in state care, 96% of them are the orphans with living parents, who are deprived of the enshrined in the UN Convention child’s right to have a family. Social stratification of the population, deterioration of living standards, weakening of the family institution has led to the increase in the number of children with the anamnesis of the early psychic trauma.
The disorder occurs more severe if the trauma is caused by human actions, rather than external factors. The most severe psychic traumas of childhood are the loss of a close adult and sexual molestation. Serious consequences are seen in the children, who suffered from the maltreatment. The emotional deprivation factors form a special group of psycho-traumatic factors [3-5].
Traumatogenic Syndrome of Mental Immunodeficiency
The yesterday’s classic stress and then - chronic psychosocial stress, today has become an existential stress
- an indispensable element of an alarming picture of the world and the way of life of almost any person.
Having become so common nowadays, thousands of demonstrations on the streets of European cities with
posters “We are not afraid” after each act of terrorism, are now accepted as almost a public recognition of the
fact that the world is ruled by terror, which has become so familiar that people are not afraid of it anymore...
That is why in mental medicine we have identified a special form of mental terrorism (MT) - destructive and
explosive manipulation of consciousness. MT continues and develops the previously developed conceptual
trend, described in terms of mobbing - bullying - crowding. The most dramatically MT is manifested in
the psychic traumatization of childhood. An epigenetic example is the unborn children of today’s migrants
in the EU, experiencing complexes of refugees with their mothers, humiliated and insulted, losing selfesteem
and self-respect, whose children may hate and despise yesterday’s benefactors of their parents, and
grandchildren are ready to blow up mentally this unbearably free world.
Prenatal traumatic experience of modern European migrants in 3-4 generations can manifest itself literally as a “mental nuclear explosion” that destroys European identity. Romantic plans for assimilation and adaptation have long since found their inadequacy.
An important epigenetic feature of the mental weapon of the modern hybrid war is that, figuratively speaking, it aims at its target in the 1st generation, clicks on the trigger in the 2nd, the ruins of yesterday’s well-being are inspected in the 3rd, and the long-term consequences become the habitual way of life for the 4th generation.
Modern chronic existential stress as a new quality of psychosocial stress through epigenetic mechanisms predetermines the activity of the genome, preparing new generations for existence in a hybrid environment - multimodal and totally socially stressful. Most of the characteristics of long-term activity of the genome are established at the stages of early development - from the prenatal period to the early maturation. It is this period that is in the focus of attention of researchers trying to explain the phenomenon of growth of psychopathology in the modern world [5-7].
The actual task is to describe and systemize the epigenetic dysfunctions of mental immunity, clinically manifested by the SMID and launching the epidemiological cascade: mental epidemic - destructive mental epidemic - pandemic of mental immunodeficiency.
Adverse experiences at an early age or an early life stress (ELS) have both acute and long-term effects on epigenetic labels in the brain that affect cognitive functions and behavior, the risk of suicide and psychic disorders throughout the life of present and future generations. The most studied in experimental neuroepigenetics are the mechanisms of histone modification and methylation of DNA [8]. The possibility of ELS induction by epigenetic modulation of gene expression leading to altered adult phenotypes has been shown [9].
In the area of a long-term neuron-synaptic plasticity [10] several regulatory mechanisms have been identified at the level of transcription and posttranscription, which include promoter activation and alternative fusion, transcript resistance and polyadenylation. New epigenetic pharmacological resources for mobilizing neural plasticity in stress disorders and neurological diseases have been revealed [10].
A study of the neurochemical profile of adult male mice subjected to traumatic stress in the early postpartum period and their offspring found that paternal trauma can also bring beneficial effects for the brain metabolism by acute stress in offspring [11]. The perspective of neuroepigenetics of PTSD, which allows identifying and predicting new candidates for neurotherapy aimed at stressful pathogenic memories, is also shown [12].
An experimental study of memory found an interesting clinical parallel. It turned out that the genes involved in the formation of memory in invertebrates are responsible for mental retardation in humans [13].
The uniqueness of the collection of memories of a person determines personal and social identity, shaping and modeling the interaction with the world. The possibility of developing new therapeutic goals for the treatment of PTSD and drug dependence by correcting the neuroepigenetic mechanisms of memory dysregulation is shown [14].
The dynamic balance between DNA methylation and demethylation of genes regulated by neuronal activity is crucial for memory processes. In a study in mice, the critical role of Tet 1 -oxidase was identified [15] in regulating neuronal transcription and maintaining the epigenetic state of the brain associated with the memory consolidation and memory chronotope. Another study shows the role of these mechanisms in the regulation of neurophysiological spatial representation and memory formation [16]. It remains an open question - how dramatic are the traces of these memories in the scale of the transgenerational models.
Emerging under stressful influence epigenetic labels fix and model the expression of gene complexes, influencing the design of the brain cell ensembles and predetermining the probability of psychic disorders [7]. It is interesting to note that an adverse transcriptional reaction to stress in the form of differential activation of the components of the immune system is more pronounced in people with a high hedonic component of mental health and significantly weaker in those whose psyche is based on the eudemonic well-being [17]. We cannot disagree with the fact that the meaningfulness of existence and the realization of one’s goals in life, spirituality and involvement in society (as opposed to hedonism and consumerism) create the best chances for realizing the life potential. That is why the biopsychosociospiritual methodology of MM allows the most complete approach to adaptive neuroengineering and self-management of mental health as a polymodal well-being.
Undoubtedly, attempting to bind certain epigenetic labels or switches to specific manifestations of behavioral phenomenology and clinical psychopathology may seem excessively mechanistic so far. The substantiation of the functional characteristics of MI accumulating epigenetic markers allows us isolating the predominantly disturbed function, which manifests itself in a certain pathoplasty and pathokinetics. Table 1 shows the clinical manifestations of MI dysfunction in the early trauma.
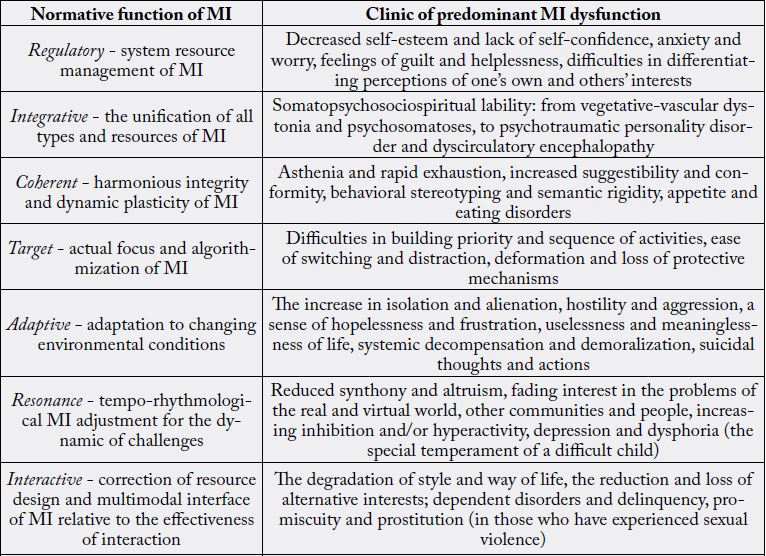
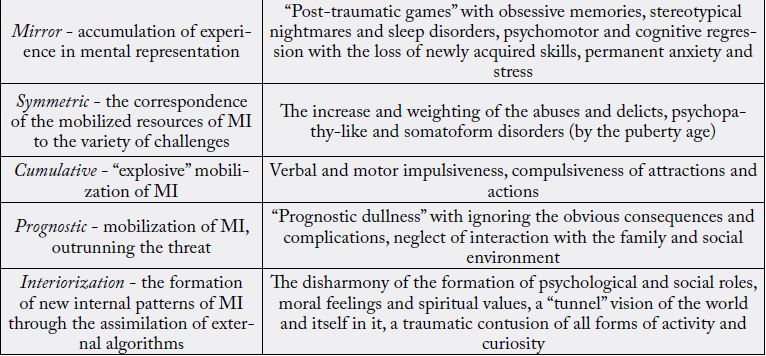
Traumatogenic SMID is represented by a variety of boundary biopsychosociospiritual identity disorders. Its pathogenetic basis consists of epigenetic accumulation of functional (reversible and dynamic) MI disorders in the “traumatogenic family”. It must be admitted that today MI is in many respects a standard placeholder, denoting the missing or indefinite multidisciplinary and multimodal parameter in the network of the relationship between genome and epigenome, identity and behavior.
Studies of early childhood psychic trauma [5,17,18] have shown the multivariance of changes in MI and biopsychosociospiritual characteristics of a “traumatogenic family” depending on the severity and duration of transgenerational stress burden. Clinical scenarios and trajectories of the destinies of new generations of “traumatogenic epigenome” essentially depended on external conditions: the same behavioral models (which are always the same for humanity) gave completely opposite effects in different social environments. This requires further multidisciplinary studies of modulation of identity and behavioral navigation based on the synergetic methodology of mental medicine.
Synergetics of the Early Psychic Trauma
The subject of synergetics are the mechanisms of spontaneous formation and preservation of complex
systems, especially in the relation to the stable disbalance with the environment (this includes all the biotic
and social organisms). The focus areas of synergetics are the nonlinear effects of the evolution of the systems
of all types, crises and bifurcation - unstable phases of the existence, involving a multiplicity of future
scenarios for further development.
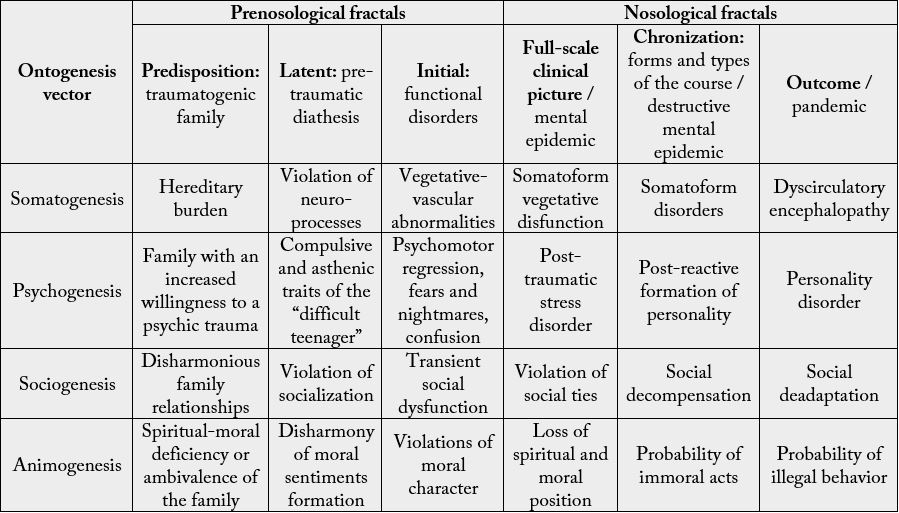
It is quite generalized and conditionally enough to present the dynamics of the early psychic trauma (EPT) from the position of the synergetic concept. Fractal dynamics is non-linear, its trajectory includes the following fractals of the biopsychosociospiritual model: predisposition, latent, initial, full-scale clinical picture, chronization and outcome (Table 2).
Feelings traumas, associated with the loss of the object of love, at first sight, seem unexpected. A study of family situations, in which the child suffered a psychic trauma, demonstrates the advanced readiness to the psychic trauma process. Here the predisposition fractal - family dysontogenesis of the traumatogenic family - begins. Unstable relation-ships, high level of emotional expression, lack of support, proneness to conflict, and hostility are the characteristic features of this family, identified with the help of projective techniques among children, who had the trauma. Lack of family traditions and spiritual values, addiction and affective disorders were observed among the parents. Low moral, educational and material levels are typical. Childrearing is held according to the type of emotional rejection and hypo-care, which entails the development of emotional and spiritual-moral deficit. Disharmony in family relationships predisposes to a distortion of moral socialization process of the child in the future.
Unfavorable hereditary burden under the influence of unfavorable factors of the environment triggers psycho-vegetative imbalance.
The following is a latent fractal of pre-traumatic diathesis (psychic diathesis is a set of features, which characterizes the predisposition to psychic pathology). In most cases, it is represented by a special temperament of the “problem child” - a very movable, in a bad mood, hardly adaptable. It is known that the more acute and massive is the psychic trauma, the lesser role is played by personal characteristics of the child. With a decrease in the severity and the intensity of the trauma, the individual characteristics become major in the formation of the clinical picture of the post-traumatic period [19]. This is especially true for the compulsive and asthenia traits. The younger is the child, the more severe are the somatic-vegetative symptoms.
Violation of neural processes is shown through the disharmony of moral feelings formation, which in future can predetermine the violation of moral socialization and development of the personality, which has low adaptive potential.
This is followed by an initial fractal of functional disorders - the actual psychic trauma. Children are more sensitive to the trauma. The younger is the child, the more dramatically the event is perceived, as the ability to assimilate and integrate the trauma in the childhood experiences is lower. After trauma, children frequently repeat the psycho-traumatic situation in games (“post-traumatic games”); there are nightmares, increased confusion, avoidance of social contacts, psychomotor regression with loss of recently learned skills, sleep disorder, the emergence of various fears [20]. This is accompanied by excessive excitability of the autonomic nervous system, high levels of wakefulness. There is a transient social dysfunction.
Vegetative-vascular dystonia and neurotic reactions are shown through the multi-variant deformation of the moral character, laying the foundation for the future development of the demoralization syndrome.
This is followed by a fractal of a full-scale clinical picture, when there are the comorbid disorders on the background of the traumatic stress disorder. Children’s behavior resembles a picture of psychopathic state. But the similarity is only superficial, because the traumatized children experience depression, anxiety, feeling of guilt, uselessness of life, suicidal thoughts. Somatic complaints increase, psychosomatic pathology is formed.
Neuroanatomical effects are shown through the decrease in volume of the hippocampus, expressed by the dextrocerebral asymmetry, decreased activity of the Broca area during the “flash-back” (perhaps, this explains why it is particularly difficult to give words to their experiences for children with PTSD [21].
Social ties are breaking, which is caused by the increasing hostility towards the world around and the lack of interest to other people’s problems.
The memory of the past is always present, but it can influence the course of life just before the bifurcation points, i.e., the decisive moments of selecting one of the possible ways of life. If the bifurcation point is passed, the path selection is done, and then the activity is determined by one of the structures of development attractors. If the traumatic past dominates over the future, and the future becomes not obvious, the fate of the trajectory is distorted.
Since the psychological past, present and future are the parts of the psychological field, both the past (past experience), and the future (expectations, desires, fears and dreams) affect the forces, which govern the individual behavior today. Psychic trauma violates this balance towards the past, creating a hostile, skeptical attitude towards the world, social estrangement, hopelessness, chronic feeling of anxiety, alienation.
Animogenesis of the somatoform dysfunction is shown through the destruction of spiritual-moral position of the child, embodied in the early development of the demoralization syndrome.
The situation is changed by the synchronized oscillations near the bifurcation point; a close adult, located nearby, who creates an atmosphere of security, changes the future. If this is not feasible, there is the chronization fractal - the postreactive personality formation, which occurs on the basis of a prolonged neurosis and is characterized by a combination of dynamic pathological changes in the character and fixed neurotic disorders. The clinical picture of this period is characterized by a combination of psychopathic-like and severe neurosis-like disorders.
Emotional disturbances of this EPT fractal are strongly colored with the somatic symptoms, which often come to the fore in the form of somatoform disorders.
In social terms, the adaptation deterioration leads to the social decompensation, and there is a risk of immoral acts in the animogenesis.
Final EPT fractal is the fractal of outcome, a personality disorder. Psychotraumatic personality disorder is formed, as a rule, not earlier than puberty age. A wide range of behavioral problems comes to the foreground. Various offences, dependence on psychoactive substances, suicidal thoughts are typical. Sexually abused girls often become prostitutes.
Somatoneurological complications of this period consist of sleep disorders, loss of appetite, eating disorders, amplification of somatoneuro-logical complaints, the development of vascular encephalopathy. Social disadaptation with a high risk of asocial personality development takes place at this stage.
Psychic traumas, experienced in childhood, form the adult destiny, which is not a priori dramatic. Traditionally, the severity of trauma and its damaging action are determined by the intensity of exposure without taking into account the surrounding circumstances. We studied the research of children of latent age, who underwent the psychic trauma in past medical history (feelings traumas, related to the loss of the love object - the death of parents, abusive treatment, sexual abuse, social orphanhood). Identified deviations of the studied parameters (intelligence, personality characteristics, “self-concept”, bioelectrical activity of brain and the artistic creativity of children) with the same nature of the trauma forced us to turn to a favorite image of the synergetics - the bifurcation model.
In the bifurcation points there is the selection of the path; the processes of another level (accidents) in the vicinity of bifurcation points can play a key role. Here such “accidents” are the circumstances related to the trauma - absence of close adult nearby, the situation of disregard, humiliation and bad care, age of the early psychic trauma till 7 years, the existence of special temperament among “problem children”, being in the orphanage, absence of professional assistance. The mechanisms, at the expense of which the psychic trauma causes psychic disorders in the remote period, include mainly the presence or absence of a close adult nearby. Close adult and traumatized child must enter into a relationship of social attraction, based on the sustainable positive feelings to each other. This means that the path of development of post-traumatic period is not the only one. If we find the right moment to intervene in the course of events, it is possible to change it.
Method for Determining the EPT Severity Degree
We have developed a method for determining the severity of the EPT, which focuses on the accidents of
near bifurcation points. Namely they determine the result of the post-traumatic period.
The algorithm of actions consists of two consecutive blocks. In the first (I) block, the nature of psychic trauma is evaluated: the short-term psychic trauma (STPT), factors of emotional deprivation (FED), chronic psychic trauma (CPT). STPT occurs among children, whose parents died as a result of a family conflict, suicide or illness (STPT-1), or which are the victims of sexual violence (STPT-2). These EPT are ranked by us with the maximum number of points - 50 and 30 points respectively (see Table 3).
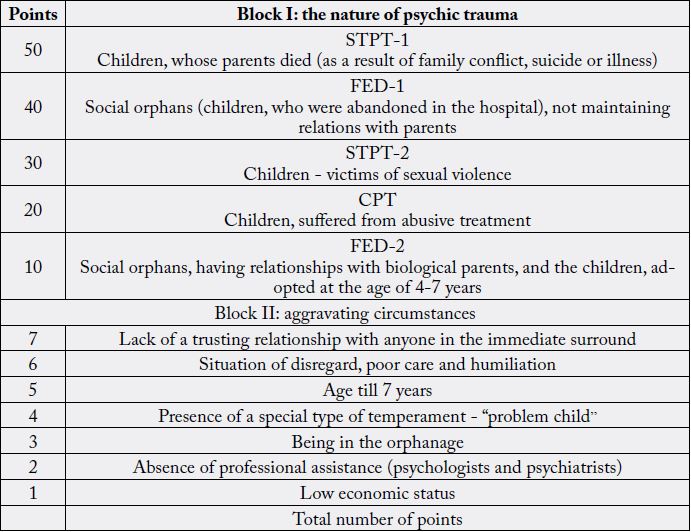
The second group, according to the EPT severity, is FED-1 (social orphans, including the children, abandoned by their parents in the hospital, having no relationship with biological parents).
CPT group (child abuse) is estimated by us in 20 points. FED-2 group (social orphans, having relationships with biological parents, and the children, adopted at the age of 4-7 years) - in 10 points.
Block II includes a list of desynchronizing fluctuations (aggravating circumstances): the lack of trusting relationship with someone in the immediate surround, the situation of disregard, poor care and humiliation, the age of trauma before seven years. The presence of a special type of temperament - “problem child” (full of play, is in a bad mood, is difficult to adapt), being in an orphan house, the lack of professional help, low economic status of the family, who are ranked on a scale from 1 to 7.
In order to determine the severity of the EPT, it is necessary to put a mark in the block 1, according to the nature of the EPT. Each case can be attributed to only one category of trauma.
Then it is necessary to evaluate the aggravating circumstances. Several aggravating circumstances can be added together, then the points of blocks I and II are added. Minimum number of points - 13, maximum - 78. EPT are divided into three groups of severity: trauma, estimated in 13-34 points, refers to mild degree; 35-56 points - to moderate; 57-78 points - to severe.
Assessment of the severity of the EPT was carried out with taking into account the nature of the psychic trauma and aggravating circumstances:
Block I (EPT nature) - STPT-1 (parents died as a result of family conflict) - 50 points;
Block II:
1. Lack of trusting relationship with anyone in the immediate surrounding - 7 points;
2. Situation of disregard, poor care and humiliation - 6 points
3. Age of EPT before 7 years - 5 points;
4. Presence of a particular temperament “problem child” - 4 points;
5. Being in the orphanage - 3 points;
6. Absence of professional assistance - 2 points.
Total score = block I points + block II points = 50 + 27 = 77 points, which corresponds to severe EPT.
Two years ago her mother was released from prison, she settled down not far from the girl, supported a relationship with her, even though they did not quite satisfy the child.
Calculation of the EPT severity:
1. Nature of the EPT - FED (social orphans, having supportive relationships with biological parents) - 10 points;
2. Age of EPT before 7 years - 5 points;
3. Being in the orphanage - 3 points;
4. Absence of professional assistance - 2 points.
According to the table of the EPT evaluation, the patient collects 20 points, which corresponds to the mild severity level.
Medico-Psychosociospiritual Care
To prevent severe consequences of an early psychic trauma, we developed a program of medicopsychosociospiritual
assistance to children, which is based on the concept of synergetics [22]. The program
consists of four blocks (see Table 4): medical and psychological, social and spiritual-moral, involving
the multidiscip-linary teams to assist with the participation of pediatricians, pediatric neurologists and
psychiatrists, psychologists, psychotherapists, social workers and teachers. Preventive measures need to begin
even in the predisposition fractal; they are aimed at improving the environment, in which a child is brought
up, ethical psychological harmonization of the parents individuality and family relations.
The latent fractal focuses on the identification of the predisposition to psychic disorders, on the diathesis diagnostics, increased stress resistance and harmonization of moral socialization of the personality.
In the initial fractal, the diagnostics of traumatic disorders becomes the most important, since in many cases they remain unrecognized and the provision of timely qualified assistance is impossible. Creating the security situation, supportive, trusting relationships with close adults, good care and professional help at this stage can reduce the negative effects, preventing the neurotic disorders among children and correcting the formation of their moral character.
In the fractal of a full-scale clinical picture, when the comorbid disorders start to appear, it is important to promote the integration of the traumatic experience into the events of the current child life; to foster the adaption to the new situation; to carry out the medicated and psychotherapeutic social and spiritual-moral correction.
The fractal of the process of chronization dictates the emphasis on the fight against social and moral exclusion with the help of psychotherapeutic and pedagogic strategies.
Fractal of the PTSD outcome - personality disorder - requires medical and psychological, social and spiritual moral rehabilitation.
Thus, the dynamics of the early psychic trauma includes the following fractals: predisposition - special traumatogenic family with increased willingness to psychic traumatization of children, being brought up in it; latent - pretraumatic diathesis; initial - traumatic stress disorder, full-scale clinical picture - neurotic and affective disorders; chronization - postreactive formation of the person; the outcome - personality disorder.
A family with an increased willingness to psychic traumatization of children differs by the unstable relationships, lack of support from family members to each other and traditions, proneness to conflict, hostility, addiction of parents, low moral, educational and material level. Pretraumatic diathesis is a borderline state, which under the influence of exogenous factors is transformed into the illness. Presence of the “problem child” temperament worsens the PTSD course. An initial period of the EPT is the actual traumatic stress disorder.
Accompanying circumstances will determine the PTSD course. Lack of close trust relations, poor care, humiliation, the age before seven years, the lack of professional assistance, staying in the orphanage - worsen the prognosis. The full-scale clinical picture includes the neurotic and affective disorders, hiding under the guise of psychopathic-like symptoms. Postreactive personality formation in the absence of favorable attendant circumstances is completed with the personality disorder.
The medico-psychosociospiritual care program for early psychic trauma, developed on the basis of the synergetic concept, includes the medical and psychological, spiritual-moral and social blocks, and involves the multidisciplinary teams in the prevention, correction and rehabilitation.
Synergetic methodology takes into account all the internal and external factors of an early psychic trauma and allows preventing its dire consequences, stopping the generalization of mental epidemic.
Conclusion
The geometric growth in the number of publications on neuroepigenetics and the rapid evolution of its
research field actualize the definition of epistemological and philosophical-gnoseological boundaries, as
well as the instrumental and technological opportunities of multidisciplinary interaction for obtaining
practically meaningful clinical results. MM is one of the newest examples of reformatting yesterday’s
nosocentric boundaries and early pre-nosological forecasting of tomorrow’s possible mental ailments. The
multidisciplinary synergetic biopsychosociospiritual methodology of MM is in demand in new discourses
of neuroepigenetics according to the mechanisms of the influence of the environment on the brain and
behavior. The substantiation for the functional lateralization of mentality (mental asymmetry) as one of
the tools of neuroepigenetic coding of identity and behavior is proposed. MM harmoniously combines in
its technological platform genetic and epigenetic molecular mechanisms, socio-psychological and clinicalpsychopathological,
spiritual-moral and religious-integrated tools. This allows MM to practically implement
yesterday’s “neuroepigenetic fantasies” about editing and formatting the design of the network cascade of genetic and epigenetic identity: molecular - cellular - tissue - organ - organism - personal - social
- population. The degree and the vector of dispersion of genomic and epigenomic identity reflect possible
resources of evolutionary variability embodied in the registers of MI and manifested by the mental resilience.
MI is a neural network multisystem and multimodal identity and consciousness interface in its interaction
with the internal and external environment. The identified 12 basic functional characteristics of MI are
modeled by epigenetic switches or labels, and are embodied in behavioral phenomenology or pathoplasty
and pathokinetics of mental disorders. The epidemic increase in the prevalence of mental and psychosomatic
disorders is suggested to be called the PMID by the name of the earliest and nonspecific syndrome of mental
immunodeficiency accumulating initial manifestations of MI dysfunctions transgenerationally. The global
predictors of PMID are many of the challenges of the modern world: from the psychic traumatization of
childhood to cumulative existential stress. The biological core of MI is the hypothalamic-pituitary-adrenal
axis, which provides epigenetic stress-modulation together with stress-sensitive areas of the brain. In MM,
sanogenetic therapy as adaptive modulation of MI triggers cascade self-renewal of personality, clinically
manifested by its therapeutic drift (diagnoses-syndromes-symptoms-states). The well-known expression of
Nobel Laureate Peter Medawar: “Genetics proposes and epigenetics disposes” should be supplemented with a
practically significant mission of MM, which embodies the design models of quality and style, the way and
meaning of life in adaptive neuroengineering and self-management of consciousness and health.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!