Biography
Interests
Fatma Hammemi1,4, Houda Ben Ayed2,4*, Makram Koubaa1,4*, Maissa Ben Jemaa2, Khaoula Rekik1,4, Maroua Trigui2, Mariem Ben Hmida2, Chokri Masmoudi3, Chakib Marrakchi1,4, Mohamed Ben Jemaa5, Emna Elleuch1,4, Imed Maaloul1,4, Sourour Yaich2, Jamel Damak1 & Mounir Ben Jemaa1,4
1Infectious Diseases Department, Hedi Chaker University Hospital, University of Sfax, Tunisia
2Community Health and Epidemiology Department, Hedi Chaker University Hospital, University of Sfax, Tunisia
3Regional Primary Health Care Directory, Sfax, Tunisia
4Extra-pulmonary Research Unity, Hedi Chaker University Hospital, Sfax, Tunisia
5Department of Orthopedics, Habib Bourguiba University Hospital, University of Sfax, Tunisia
*Correspondence to: Dr. Houda Ben Ayed, Community Health and Epidemiology Department, Hedi Chaker University Hospital, University of Sfax, Tunisia.
Copyright © 2018 Dr. Fatma Hammemi, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Despite preventive measures, tuberculosis (TBC) is still a public health problem worldwide.
Osteoarticular tuberculosis (OATBC) requires an early diagnosis and an effective treatment in
order to limit complications and sequelae. In our country, recent and exhaustive OATBC data are
scarce. In this perspective, we aimed to study the epidemiological, clinical and evolutionary features
of OATBC.
We conducted a retrospective study including all patients with TBC in Southern Tunisia between
1995 and 2016.
Totally, we enrolled 181 cases of OATBC. There were 93 females (51.4%). The mean age was 47 ± 20
years old. The main site was spondylodiscitis in 131 cases (72.3%). The mean duration of treatment
was 12±5 months. The disease evolution was favourable in 143 cases (80%). In comparison with
other forms of extra pulmonary TBC, patients aged 60 years and above were significantly more
affected by OATBC (Odds ratio (OR) = 2.4; p < 0.001). OATBC was significantly more frequent in
rural areas (OR = 2; p < 0.001). The treatment duration was significantly longer (12.2 ± 5 vs 9 ± 3.6
months; p < 0.01) than the other TBC sites. As for the disease evolution, relapse was significantly
more frequent in OATBC patients (OR = 6; p < 0.001), while recovery was significantly more
frequent in the other sites of extra-pulmonary TBC patients (OR = 0.5; p = 0.01).
OATBC was ranked at an alarming rate in our region. Despite an adequate treatment, the prognosis
was more severe in comparison with other extra pulmonary tuberculosis sites, particularly among
elderly. An early diagnosis and a regular follow-up are highly recommended in order to avoid severe
forms and sequelae.
Abbreviations (if used)
TBC: Tuberculosis; OATBC: Osteoarticular tuberculosis; IQR: Interquartile range; OR: Odds ratio; EPT:
Extrapulmonary Tuberculosis.
Introduction
Tuberculosis (TBC), an infection caused by Mycobacterium, is a public health problem worldwide. In 2016,
an estimated 10.4 million patients were newly diagnosed with TBC and 1.7 million were dead from TBC
[1].
Despite preventive measures, the WHO estimated that tuberculosis incidence increased in Tunisia through these few last years from 26/100000 inhabitants in 2000 to 38/100000 inhabitants in 2016 [2]. This increase was almost due to a rise in extra-pulmonary TBC cases (EPT), while pulmonary TBC cases had remained almost the same [3]. Actually, TBC is a multisystem disease that typically affects the lung, but can also affects any organ or tissue, such as the bone, which is considered as an unusual site. Osteoarticular TBC (OATBC) accounts for 1-3% of all forms of TBC [4]. Clinical symptoms are unspecific, which explains the diagnosis and treatment delay. Therefore, it should be bearded in mind in front of a chronic bone or joint disease. The most common site is the spine, followed by extra-spinal TBC, which is less frequent.
In our country, recent and exhaustive data of OATBC are scarce. Studying its epidemiological particularities over time would be of a great benefit for policymakers to prioritize preventive interventions accordingly. In this perspective, we aimed to study the epidemiological, clinical and evolutionary features of OATBC in South of Tunisia.
Materials and Methods
We carried out a retrospective study including all patients diagnosed with TBC over a 22-year period
between 1995 and 2016 in South of Tunisia.
Data were collected from the regional TBC register of Southern Tunisia on pre-established sheets. We
included all new cases of TBC, all ages combined. At enrolment, we excluded patients who were lost to
follow up or relapsing. Diagnosis was based on bacteriological and /or histological proof. In default, it was
based on strong clinical evidence, followed by an adequate response to antitubercular treatment. A favorable
evolution of the disease was defined by a recovery from OATBC without relapse or complication occurrence
during the follow-up.
Statistical analysis was performed using SPSS.20. Qualitative variables were presented as numbers and
percentages. Quantitative variables were carried out by means and standard deviation if they were normally
distributed. Otherwise, medians and interquartile ranges (IQR) were performed. We used Chi square test to
compare two frequencies and Student test to compare two means in independent samples. We considered
the difference between the groups significant when p<0.05.
Results
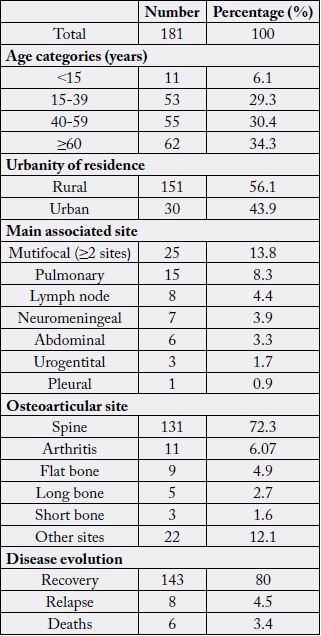
During the study period, we identified 181 patients with OATBC among 1711 patients with EPT (10.6%),
representing 6.4% of all TBC cases. Of all TBC cases, we noted 93 females (51.4%). The mean age was 47 ±
20 years old. Sixty-two patients (34.3%) were aged over 60 years old and 11 patients (6.1%) were aged less
than 15 years old. According to residency, 101 patients came from a rural area (56.1%). Multifocal TBC was
noted in 25 cases (13.8%). We identified 15 cases (8.3%) of OATBC with concomitant pulmonary TBC.
Other EPT sites associated to OATBC were mostly represented by lymph node TBC in 8 cases (4.4%)
and neuro-meningeal TBC in 7 cases (3.9%). The main site of OATBC was spondylodiscitis in 131 cases
(72.3%). We noted 11 cases (6.07%) of arthritis, among whom hip TBC were noted in 5 cases (2.76%),
followed by knee TBC in 2 cases (1.1%). Treatment regimen was based on fixed drugs combination in 38
cases (21%).
The mean duration of treatment was 12 ± 5 months. The disease evolution was favorable in 143 cases (80%). We noted 8 relapsing cases (4.5%) and 6 deaths (3.4%) during the follow up (Table1).
Patients aged 60 years and above were significantly more affected by OATBC (Odds ratio (OR) = 2.4;
p<0.001). Furthermore, OATBC was significantly more frequent in rural areas (OR = 2, p < 0.001).
Comparison of the disease evolution showed that relapse was significantly more frequent in OATBC
patients (OR = 6; p < 0.001), while recovery was significantly more frequent in other sites of EPT patients
(OR = 0.5; p = 0.01). The treatment duration was significantly longer in OATBC patients (12.2 ± 5 vs 9 ±
3.6 months; p < 0.01). As to gender, treatment regimen and mortality, no significant difference was noted
(Table 2).
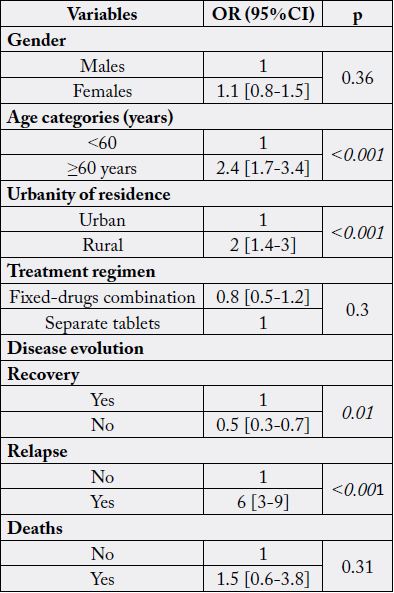
OR: Odss Ratio ; 95% CI : 95% Confidence Interval
Discussions
Our study highlighted the substantial burden of OATBC in Southern Tunisia, accounting for 10.6% of all EPT cases. In China, it represented 10% of all EPT cases and was ranked third most common site after pleural and lymph node TBC [5]. As for Turkey, it was ranked fourth, representing 7.4% of all EPT cases [6]. Furthermore, among all sites, OATBC represented 6.4%, which was consistent with results noted in England, where it represented 6.7% of all TBC cases [7].
According to age categories, our study showed that patients aged 60 years and above were significantly more affected by OATBC, comparing to other EPT sites. This might be explained by the diagnosis delay noted in OATBC. Patients may suffer from back pain for years and do not even consult. However, in comparison with other countries, researches showed that young adults were mostly concerned in endemic areas. The same results were noted in China with a mean age of 44 years old for OATBC patients [5]. However, in developed countries, a bimodal age distribution was noted. The immigrant patients were young adults, whereas the native ones were elderly patients aged over 60 years old [8].
In India, a study reported that the most common site was the spine [9]. In fact, TBC, the result of reactivation of quiescent bacterium following a deficiency of the immune system, is transmitted by the respiratory tract. Then, Mycobacterium, through the blood circulation, reached other parts of the body such as the spine which is considered as a target for it [9,10]. In our study, we found a predominance of spondylodiscitis which was concordant with researches in other countries, such as India [9]. The hip was the second most common site of OATBC, followed by the knee, which was consistent with results noted in previous reported studies [11]. Regardless of its site, TBC caused a chronic infection and might lead to a serious damage if it was not diagnosed and well treated in time. The WHO recommended 9 months for treatment of OATBC [4]. However, in our study, a longer duration was noted. The median duration of anti-tubercular therapy was significantly longer, compared to other EPT sites. This might be explained firstly, by the site itself, since OATBC, as well as neuro-meningeal and miliary TBC, were considered as a severe form of TBC and secondly, by the diagnosis delay, which was responsible for advanced and complicated forms of the disease. The treatment was basically starting with quadri-therapy for 2 months, followed by a bi-therapy for the rest of the period, which was consistent with a French study reporting that 14.7 and 13 months were the mean durations of treatment in spondylitis and non-spondylitis TBC, respectively [12].
Another interesting finding in our study is that OATBC was significantly more frequent in rural areas. This might be related to the low socio-economic level and to the reduced financial input for TBC diagnosis and treatment in limited-resources areas. Therefore, policymakers should maintain an equitable distribution of healthcare services between rural and urban areas, by allocating affordable resources according to the geographical distribution and the effective needs of patients.
As for the disease evolution, relapse was significantly more frequent in OATBC patients in comparison with other sites of EPT patients. This might be related to the diagnosis and treatment delay or its insufficient duration. It be explained also by TBC and brucellosis co-infection which could be not even diagnosed.
Conclusions
Osteo-articular tuberculosis is still endemic in Southern Tunisia. Despite an adequate treatment, the prognosis
was more severe in comparison with other EPT sites, particularly among elderly. An early diagnosis, an
antitubercular therapy for the appropriate duration and a regular follow-up are highly recommended in
order to avoid severe forms and sequelae.
Figures
Not applicable.
Supplementary Files (if applicable)
Not applicable.
Acknowledgements
Not applicable.
Conflicts of Interests
No conflict of interest.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!