Biography
Interests
Hosein Najafpour1 & Bahram Alamdary Badlou2*
1SONAPS Clinic. Research and Development Dept., Tehran, Iran
2BBAdvies and Research, Research and Development Dept., Zeist, The Netherlands
*Correspondence to: Dr. Bahram Alamdary Badlou, BBAdvies and Research, Research and Development Dept., Zeist, The Netherlands.
Copyright © 2021 Dr. Bahram Alamdary Badlou, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
History
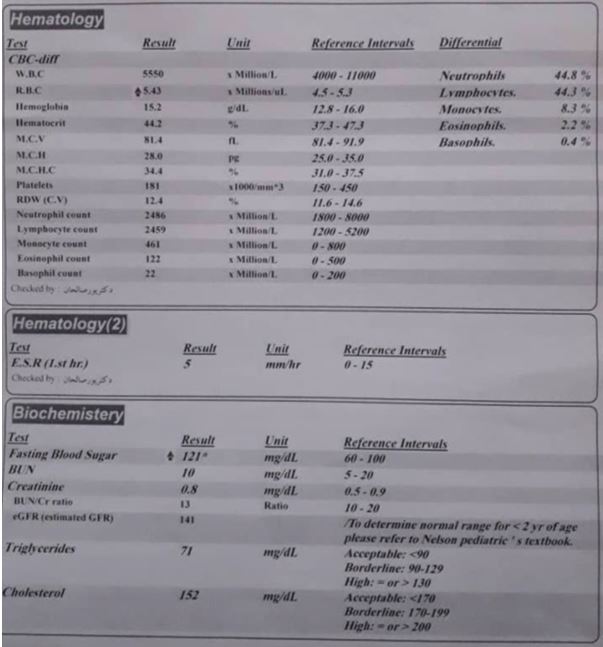
Here we report an exceptional case of a Persian young man 14 years old Mr. Ali.T who under sudden
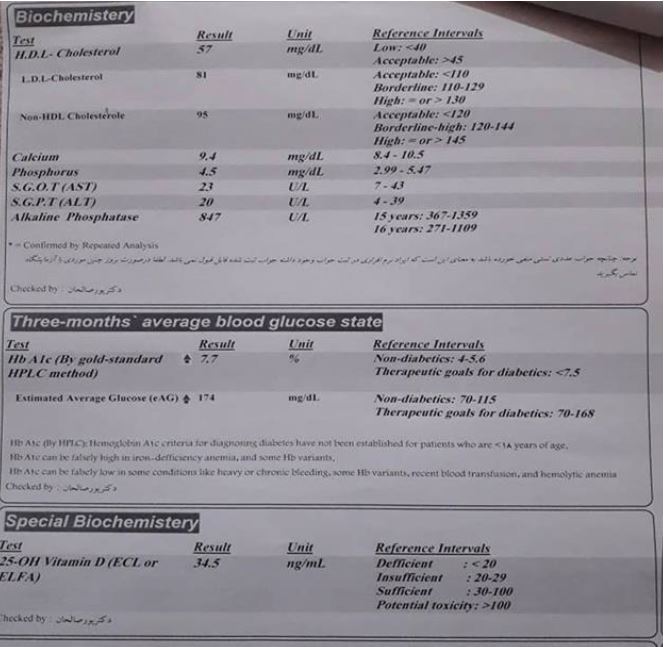
distress, Erythrocytosis (fig 1), increased HbA1C and glucose levels in the last three months (fig 1,2),
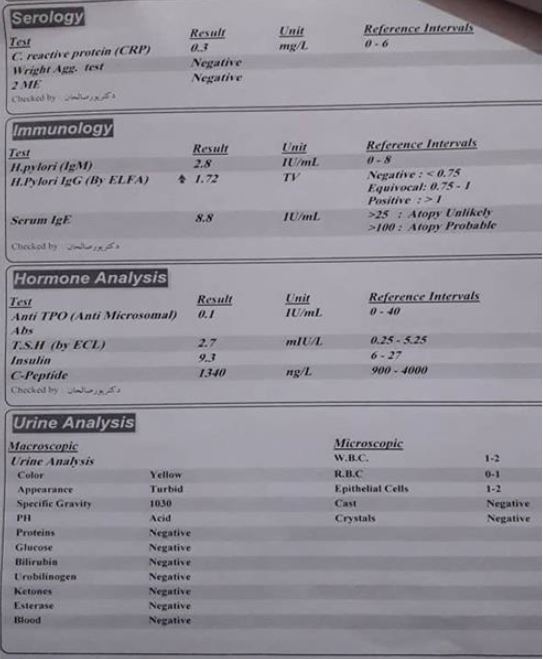
possible H. Pylori infection and inflammation but normal fatty acids, Triglyceride, and Cholesterol levels
(fig 3), got Diabetes Mellitus type 1 (DMT1) diagnosis (fig 1-3) and insulin-dependent treatments with 2
insulin injections subcutaneous daily (60 injections per month) with some symptomatic food allergies, visit
our practice in May 2020, in Tehran, Iran.
After our Medical team visited diagnostics and treatments (D&T), we did succeed to change our case’s metabolism as such, which our D&Ts caused his whole insulin metabolism was changed, considerably. Our D&Ts previously changed another patient’s metabolism and restored her complex cyanotic tetralogy of Fallot [1]. Besides, our case who DMT1 was confirmed, in less than 24 hours become independent of insulins’ injections, however. Moreover, we did succeed to decrease his Insulin injections frequency, considerably.
Physical Examinations
A 14-years old Persian young thin man presented with DM1 disorders increased HbA1c and glucose in the
last three months’ checkups, potential gastrointestinal tracks and hematologic inflammation and H.Pilory
chronic infection were generally chronic-related distressed with anxiety for treatments, and with glucoseand,
not fatty acids ‘metabolic syndrome showed increased systemic HbA1c levels in the last two months.
Our SONAPS diagnostic and associated treatments and diet-related approaches showed remarkable signal
transduction disorders in the Vagal nervous system associated with central nervous systems (CNS) and (co)
related brain-gut-heart axis leakages.
Lesson Learned
Known is that DMT1 is an irreversible metabolic disease, which could potentially progress toward severe
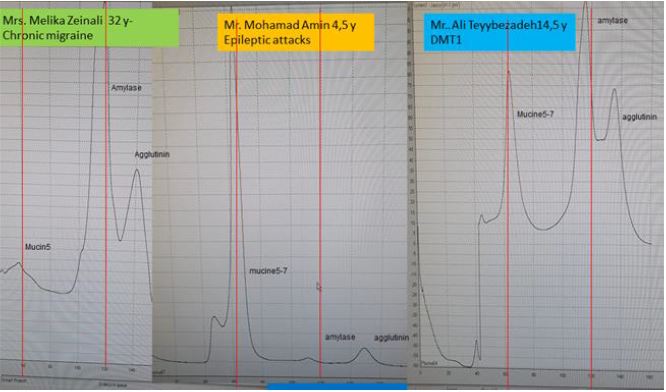
insulin-dependent metabolic disorders and an increase in morbidity and mortality rates. The Saliva amylase
overproduction (originating from Saliva-Kidney-GIT axis) and associated side effects might chronically
result in the DMT1 (ir-)reversibly [1-5]. Where does serum amylase come from? and what is the mechanism
of amylase production/recirculation/clearance disorders? are not completely elucidated yet. Moreover, recent
data are suggesting that the serum amylase concentration redirects the equilibrium between the rates of
amylase entry into-, and removal from the systemic blood circulation [3-5]. The pancreas and salivary glands
have amylase concentrations that are several orders of magnitude greater than that of any other normal
tissue, and these two organs probably account for almost all of the serum amylase activity in normal persons
[4-8].
Recall, the Pancreatic hyperamylasemia might be resulted from an offense to the pancreas, ranging from trivial cannulation of the pancreatic duct to severe pancreatitis [4-8]. Hyperamylasemia due to salivarytype isoamylase is observed in conditions involving the salivary glands, as we also reporting in our case here (fig 4). In addition, this type of hyperamylasemia occurs in conditions, in which there is no clinical evidence of salivary gland diseases, such as chronic alcoholism, postoperative states (particularly postcoronary bypass), lactic acidosis, anorexia nervosa or bulimia, and malignant neoplasms that secrete amylase [4-8]. Hyperamylasemia can also result from decreased metabolic clearance of amylase due to renal failure or macroamylasemia [4-8]. Moreover, in our case Mr. Ali T. now 15 years old showed healthy kidney and glomerular filtrations during last years’ checkups.
Taken together, in our case either with combination of our in-house developed SONAPS as described [1], and/or with personalized diagnostics i.e allergic diet restrictions, adjustments of recommended appropriate diet supplements, personalized medical consult: not only significantly decreased the degree of Insulin injections frequency, but also did decrease his distressed condition, remarkably. Although, because of distance and limited access of patient to first degree Medicare and Medicaid he did fall back to insulin-dependent condition again, however. More in detail investigation in near future needed to unravel what we exactly done that made him insulin-independent.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!