Biography
Interests
Mustafa Hussein
Faculty of Medicine, University of Medical Sciences and Technology (UMST), Khartoum, Sudan
*Correspondence to: Dr. Mustafa Hussein, Faculty of Medicine, University of Medical Sciences and Technology (UMST), Khartoum, Sudan.
Copyright © 2021 Dr. Mustafa Hussein. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Female genital mutilation (FGM) is the act of cutting part(s) of the female genitalia for nonmedical
reasons. It is practised in 30 countries globally, affecting at least 200 million girls and
women. Sudan is one of the countries where FGM is prevalent, having its social and cultural
driving forces. The objective of this study is to identify the interventions and programmes that have
been implemented to address FGM in the country.
A scoping review based on Arksey and O’Malley framework was carried out to identify published
papers on interventions to address FGM in Sudan. Eligibility criteria included work published in
English primarily addressing FGM strategies or interventions in Sudan. Strategies implemented
elsewhere were omitted.
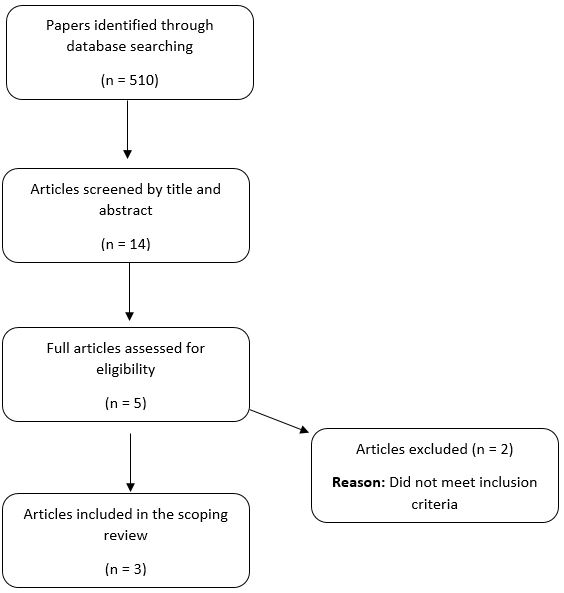
A search of the electronic databases using the keywords identified 510 documents. Scanning by article title and abstract yielded 14 papers, out of which 5 were full reviewed. Out of the full reviewed papers, 3 met the inclusion criteria.
The interventions addressed FGM through three major themes: (I) Knowledge and awareness,
(II) Attitude change and (III) Social norms. Each of the implemented strategies was able to yield
favourable outcomes in terms of increasing knowledge and awareness towards FGM, bringing
attitudinal change and reducing the pro-FGM social norms.
Review of the literature revealed paucity in the interventions addressing FGM in a country where
the practice has its deep roots. The efforts of research institutes and organisations in formulating
strategies to curb the spread of the practice in the country are highly appreciated. However, there is
still a wide margin of improvement that researchers can work on.
Introduction
Female genital mutilation (FGM) is the act of cutting part(s) of the female genitalia for non-medical reasons. It is sometimes referred to as female circumcision or cutting. According to the WHO, “it comprises all procedures that involve partial or total removal of the external female genitalia, or other injury to the female genital organs for non-medical reasons” [1]. It is practised in 30 countries globally, affecting at least 200 million girls and women [2].
In a joint statement issued by the WHO, UNICEF and UNFPA, FGM has been classified into four types:
• Type I - involves the partial or total removal of the clitoris and/or the prepuce (clitoridectomy)
• Type II - constitutes the partial or complete removal of the clitoris and the labia minora, with or without
the excision of the labia majora
• Type III - comprises narrowing of the vaginal orifice with the creation of a covering seal by cutting and
positioning of the labia minora and/or the labia majora, with or without excising the clitoris. This type is
also referred to as infibulation.
• Type IV - includes all other harmful procedures to the female genitalia for non-medical reasons, such as
pricking, piercing, incising, scraping and cauterisation [3].
In Sudan, the practice has its social, cultural and religious driving forces. In some societies, FGM is practised to preserve virginity and prevent premarital sexual intercourse. Thus, bringing honour to the family. Also, it is thought to be a sign of beauty and cleanliness. Besides, it is perceived to enhance the male partner’s sexual pleasure [4].
In a cross-sectional survey, it was noted that the pro-FGM attitude was more prevalent among the uneducated individuals residing in rural settings and who have a high sense of tribal identity [5]. This observation had been noted earlier by Toubia, who suggested that the prevalence of FGM tends to follow a tribal and ethnic rather than national affiliation [6].
The idea that FGM is a social norm has been a major contributing factor to the persistence of the practice. Surveys revealed that some families put their girls through the painful experience to avoid being socially labelled and stigmatised. Mackie suggests that people continue to practise female circumcision since it is a prerequisite for marriage [7].
In 2000, the WHO estimated the prevalence of FGM in northern Sudan to be 90% [8]. In 2014, a multiple indicator cluster survey showed that 86.6% of females between the age of 15 to 49 years have been victims of the procedure [9].
Some health campaigns have been launched to help in tackling female genital cutting in Sudan. The efforts of which are considerable. In this paper, we aim to overview the preventive and response strategies that have been implemented to address FGM in the country.
Methodology
A scoping review of the existing literature was conducted. This was based on Arksey and O’Malley framework that comprises the following steps:
I. Identifying research question
II. Identifying relevant studies
III. Selecting significant studies
IV. Charting the relevant data
V. Summarising and reporting the results [10].
The research question was “What are the preventive and response interventions that have been implemented
to address female genital mutilation in Sudan?”. We searched the literature in electronic databases between
January and March 2021 to find the relevant publications. These databases included PubMed, Medline and
Google Scholars. The keywords used were ‘female genital mutilation’ and/or ‘female genital cutting and/or
‘female genital circumcision’ and ‘Sudan’.
For identifying the relevant literature, inclusion and exclusion criteria were developed. Criteria included
work published in English primarily addressing FGM strategies or interventions in Sudan. Strategies implemented elsewhere were omitted. Documents such as conference proceedings and book reviews not
relating to the subject under study were also excluded.
A search of the electronic databases using the keywords identified 510 documents. Scanning by article title
and abstract yielded 14 papers, out of which 5 were full reviewed. Out of the full reviewed papers, 3 met the
inclusion criteria. The 2 excluded papers were Johansen R et al. (2013) [11] and Johansen R et al. (2018) [12].
The final 3 papers included in the scoping review were Mahgoub et al. (2019) [13], Vogt et al. (2016) [14]
and Evans et al. (2019) [15]. The scoping review process is demonstrated in figure 1.
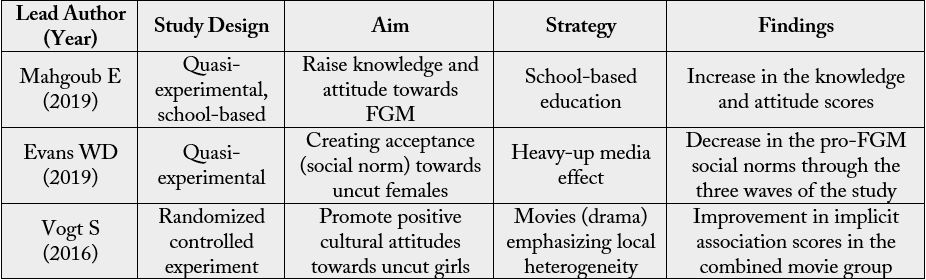
The data were charted using the lead author name, publication year, study design, aim, strategy and findings.
Besides, the results were summarised thematically.
Results
The results are presented under three themes: (I) Knowledge and awareness, (II) Attitude change and (III)
Social Norms. These are based on the aim or objective of the implemented strategies.
Mahgoub et al. conducted their intervention among secondary school students in Karary locality, Khartoum
State. Two schools were randomly selected and then two second grade classes (out of four classes) in each
school were also randomly chosen.
In their programme, Mahgoub et al. attempted to increase the knowledge and attitude of female teenagers through a school-based intervention strategy. The programme was divided into three phases: pre-intervention, intervention and post-intervention phases. A structured, close-ended, self-administered questionnaire was used to collect data during the pre and post-intervention phases. The intervention phase included health educational lectures, group discussions and video display. The post-intervention phase was carried out six weeks later.
The knowledge of the students about type I, II, III and IV FGM significantly increased from 29.2%, 17.5%, 8.4% and 27.3% in the pre-intervention phase to 81.3%, 75.8%, 49.3% and 67.8% in the post-intervention phase. The student’s knowledge about complications from FGM also followed a similar trend. A scoring system was created to reflect on the student’s overall knowledge. The means of knowledge score increased from 8.63 (SD ± 2.562) to 11.99 (SD ± 2.264) in the pre and post-intervention.
Vogt et al. intervention was directed towards changing the cultural attitudes towards FGM. Their strategy
relied on the influence of entertainment. The intervention was carried out in two experiments, one at the
individual level and the other at the community level. It was conducted at Gezira state.
Four telenovela-style movies were produced and shown to people in two fully randomized and controlled experiments. The first movie discussed the intrinsic factors associated with FGM “values movie”. The second movie was about marriageability concerns. The third was a combination of the first two themes, and the fourth was a control. The control movie included only the main plot, while the other three had subplots related to FGM.
At the individual level, the three experimental movies produced a positive attitude change for uncut girls among 66.7 - 72.9% of the participants compared to 35.6% in the control group. The second experiment showed significant improvements in attitude towards uncut girls as defined by the implicit association scores. However, this improvement was confined to the combined movie group.
The authors also noted three significant findings. The first is that programmes that take local heterogeneity as a starting point have the potential to positively change cultural attitudes. The second, addressing individual values and marriageability together can produce attitudinal change that lasts longer rather than discussing them separately. And the third is the positive role that entertainment can play in the efforts to abandon the practice [14].
The strategy of Mahgoub et al. also aimed to bring attitude change towards FGM. This was evident in the attitude scores that improved from 5.76 (SD ± 1.937) in the pre-intervention to 6.53 (SD ± 1.164) in the post-intervention. However, the authors acknowledge that educational campaigns alone are not sufficient to maintain attitude and behavioural changes towards an issue of great sociocultural complexity.
Evans et al. addressed FGM in the context of social norms. Thus, their intervention relied on Social Norms
Theory to create acceptance towards uncut girls. They launched a campaign labelled “Saleema” across the
different states of the country. The word “Saleema” connotes remaining whole and healthy in body and
mind, unharmed and in a God-given condition [16]. A number of local and international organizations
participated in this campaign, including UNICEF, National Council for Child Welfare, Ahfad University
for Women (AUW) and Gender and Rights Advocacy Centre (GRACe).
The study design was a quasi-experiment carried across the 18 states of the country. It received approval from AUW Research Ethics Board and UNICEF Procedure for Ethical Standards in Research in October 2015. Data were collected at three waves. Pre-test data was collected in December 2015. The second and third waves were in December 2016 and 2017, respectively. The intervention included four main activities:
1. Sufara Saleema Campaign
2. Saleema Colours Campaign
3. Community Dialogue
4. Born Saleema Project
These activities aimed to address FGM from different angles. This included a public pledge to end the practice, dialogue on the existence of the practice, celebrity endorsement and a pledge not to cut newborn daughters immediately after birth.
The authors used a heavy-up effect between the second and third phases of data collection. This involved increasing the dosage of the activities of the campaign nationwide. The heavy-up effect is a media and advertising research method in which campaign implementation activities are increased over time by a known quantity to evaluate its impact on outcome [17].
A two-stage cluster sampling was carried out. In the first stage, a sample of clusters (primary administrative units) was drawn from the 18 states. This was done use Proportion to Population Sampling. In the second stage, 26 households from each cluster were selected through systematic sampling.
Two measurement tools were used for evaluation. One was independent and the other self-dependent. The authors developed Saleema Evaluation and Monitoring System (SEAMS) which is an independent (exogenous) assessment tool. The staff of the State Councils for Child Welfare were trained on data collection. It was uploaded to the database on a monthly basis.
The second assessment tool was a questionnaire to assess awareness, message receptivity, subjective and descriptive norms and related knowledge, attitude and behaviour. The questionnaire was administered by GRACe interviewers.
All data from the 3 study waves were compiled into a single datasheet. Confirmatory factor analysis (CFA) across the different themes was carried out. Factor loading and Chronbach’s alpha (> 0.6) test were used to assess factor strength.
The total sample size at wave 1, 2 and 3 were 3,720, 3,724 and 3,824, respectively (11,268 in total). Females represented 55% of the sample size, and the mean age was 38.3 years.
There was a wide variation in the number of events and attendance by state. North Darfur had a mean percapita attendance of over 41 persons per event, while Sennar had a mean of less than 1. Overall, logged, per-capita attendance increased by 65% between wave 2 and 3.
Saleema event participation for each state was investigated and regression analysis conducted for logged, per-capita attendance. Improved knowledge, attitude and behaviour towards uncut girls were positively correlated with attendance at wave 3.
There was a gradual decline in pro-FGM social norms through the three waves of the study. Social norms agreement factor decreased from 1.59 at wave 1 to 1.43 at wave 2 to 1.40 at wave 3 (lower scores desirable).
Social norms CFA based on SEAMS was appropriate with an overall alpha scale of 0.8274. Multivariate regression analysis of self-reported exposure to the Saleema campaign showed improved anti-FGM social norms at wave 3 (coeff. = - 0.329, p < 0.001). The improvement was dose-responsive, with an increase in event exposure between wave 2 and 3 being associated with greater improvement in social norms factor (coeff. = - 0.146, p < 0.001).
Some variables were associated with lower pro-FGM social norms. These included being male, advanced age, education beyond secondary school and being unmarried.
A summary of the results is presented in table 1.
Discussion
Mahgoub et al. programme focused on secondary school girls. Excluding males from an intervention to
tackle FGM in a country where it is highly prevalent can hold back the implemented efforts. Many studies
in the literature highlighted that fathers and grandfathers are less in favour of carrying out the practice as
compared to mothers and grandmothers [18,19]. Generalizability of the results would also be an issue as the
intervention was conducted among secondary school girls in one locality in Khartoum State.
Vogt et al. highlighted the positive influence media can have on changing cultural attitudes towards FGM. A significant finding of this programme is that endorsing local heterogeneity is the first step to bring attitude change. To avoid contamination that could have occurred between the study participants in the first experiment, cluster randomization was carried out in the second experiment. Thus, entire communities were randomly allocated in the second experiment.
Evans et al. tackled FGM from a different perspective. Rather than raising awareness about the negative consequences of the practice and promoting attitudinal change, they attempted to promote acceptance towards uncut girls. Thus, indirectly raising awareness and promoting attitudinal change. This was addressed through the Saleema campaign that relied on Social Norms Theory.
We can see that there is an evident discrepancy in terms of resources and support between Saleema and the other two interventions. Saleema was carried out across all 18 states of Sudan and adopted four different levels of approach. Different local and international stakeholders provided support and expert assistance to the campaign.
All the identified research were preventive interventions to address FGM in Sudan. No response interventions to help females who are victims of FGM had been identified, although it is important, as the practice has its physical and psychological complications. Some victims can suffer from the sequelae of FGM for long periods. We identified one case report that describes the role of reconstructive surgery in restoring anatomy and improving sexual function in a young lady with FGM [20].
In a country where more than 86% of females between the age of 15 to 49 years have had FGM [9], the number of interventions addressing it is far below what is expected. Although search and language capacities could have been a limitation, paucity in published research reflects a wide gap that needs to be addressed.
Conclusion
FGM is a form of violence against women and an issue of child protection. The efforts of research institutes
and organisations in formulating strategies to curb the spread of the practice in the country are highly
appreciated. However, there is still a wide margin of improvement that researchers can work on. Presence
of a robust legislative power that criminalises it is a fundamental domain in curbing its spread. In 2005,
Sudan signed the Maputo Protocol adopted by the African Union to end the practice in the continent
[21]. Interestingly, Sudan has been the first African state to criminalise FGM since 1924 [22]. However,
the legislation concerns type III only. In reviewing the literature, we can find that there is a paucity of
interventions focusing on the psychological aspect of FGM victims. Furthermore, few case reports have
discussed the effects of reconstructive surgery.
Disclosure Statement
The author has no conflicts of interest to declare
Author Contributions
Hussein M conceived the idea and screened the titles and abstracts of all documents based on the inclusion
and exclusion criteria. The final five articles were fully reviewed, and three of them that met the inclusion
criteria were included in the scoping review.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!