Biography
Interests
Catovic, A.1*, Pleho-Kapić, A.2, Voljevica, A.3 & Custovic, A.4
1Department of Hygiene, Faculty of Medicine, University of Sarajevo, Bosnia and Herzegovina
2Department of Pathophysiology, Faculty of Medicine, University of Sarajevo, Bosnia and Herzegovina
3Department of Anatomy, Faculty of Medicine, University of Sarajevo, Bosnia and Herzegovina
4Faculty of Medicine, University of Sarajevo, Bosnia and Herzegovina
*Correspondence to: Dr. Catovic, A., Department of Hygiene, Faculty of Medicine, University of Sarajevo, Bosnia and Herzegovina.
Copyright © 2021 Catovic, A., et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Some diet patterns are connected with a higher risk of a chronic disease, at times due to changed ratio between some nutrients. The objective of this study was to determine the content of sodium and potassium contained within the meals of students of Faculty of Medicine over a period of three days. The cross-sectional study included sample of 44 students that were introduced in the CINDI dietary guide. Students were divided into two groups. First group, comprised of 20 students took part in the study during December 2015, and the other group of 24 students took part during April 2016. The data about students’ diet was collected in two ways - through FFQ and through dietary food recall. The average intake of sodium and potassium was estimated using Nutritional analysis computer program (Nutrics Professional Nutrition Analysis Software). Average estimated sodium intake was 2042.20±905.83mg for males and 1500.25±533.92mg for females. Average estimated potassium intake was 2828.60±623.30mg for males and 2244.38±580.54mg for females. Average Na/K ratio of 0.72 for males, and 0.76 for females. These results emphasize the importance of choosing healthy food to achieve adequate nutrient intake, as well as the importance of appropriate servings from chosen food.
Abbreviations
AI - Adequate Intake
BMI - Body Mass Index
CDRR - Chronic Disease Risk Reduction
CINDI - The countrywide integrated noncommunicable disease intervention
FFQ - Food Frequency Questionnaire
SD - Standard Deviation
WHO - World Health Organization
Introduction
Nutrition is a major modifiable determinant of chronic diseases. Epidemic proportion of obesity, diabetes,
cardiovascular diseases, cancer, osteoporosis, and dental diseases can be explained by transfer of risk behavior
from one population to another. In the second half of the twentieth century transitions in nutrition have
been introduced. There are some shifts in the post-World WarI 1period in the patterns of diet that can be
named as “modern” dietary patterns. Analyses of economic and food availability data for 1962-1994 [1]
revealed that the diet structure has shifted to high-fat, energy-dense diets. One of consequence with great
impact on human health has been replacement of fruit and vegetable by animal-based foods [2]. Increased
consumption of sugar and sweets, sweetened beverages, fast food, red meat, and processed food is described
as the “westernization” of the diet [3]. The shifts in global dietary habits and food consumption trends could
be explained by the impact of rapid urbanization [1] and poorer diet quality is observed in a diet during the
transition from adolescence to adulthood [3]. Besides qualitive changes in a diet, there are also quantitative
changes that are reflected in some of the specific dietary components like sodium and potassium. The mean
sodium intake varies by population. The higher sodium intake ranged from 2.07 to 4.77g/day [4]. The
average potassium consumption in many countries is below 70-80mmol/d (2,730-3,120mg/d) [5]. In the
typical US diet the average potassium content is 2,620mg, and average sodium content is 3.27g/d [6]. High
amount of sodium in diet is due to the use of table salt, as well as a high intake of processed foods (with
added salt) [4,6]. Potassium-rich foods are fruit and vegetables [5,6]. It has been estimated that the so-called
Paleolithic diet delivered about approximately 10,500 milligrams of potassium a day and under 700mg of
sodium, and produced a Na/K ratio of 0.07 (1/15). Potassium sources were fruits, vegetables, leaves, flowers,
roots, and other plant sources [7]. The scarcity of sodium is reflected in kidneys ability to hold onto this
nutrient. Sodium retention increases intravascular volume, and thus increases blood pressure, damaging
blood vessels and causing vascular dysfunction [8]. Modern diet pattern lacks in fresh food and is abundant
with food containing sodium chloride (NaCl). As a result, the ratio of sodium to potassium in modern
diet has changed to 1-to-1, and verse to 3:1. This can be found even in cases when intake of potassium is
equal to recommended level [9]. Sodium and potassium are classified as essential nutrients. Both minerals
are required in small amounts for normal cell functions and for maintaining fluid and electrolyte balance.
According to WHO guidelines adults should consume less than 2,000mg of sodium, and at least 90mmol (3,510mg) of potassium per day [4,5]. Based on a comparison of these recommendations the adequate range of dietary Na/K ratio is up to 0.57 according to WHO recommendation.
Data on sodium and potassium intake in the diet in Bosnia and Herzegovina are limited. According to country profile of Bosnia and Herzegovina there was a fruit and vegetable supply (2009 year) of 822 grams per capita per day [10] and mean population salt intake for adults aged 20+ (2010 year) was 9g/day [11]. Based on data collected during the 2011/12 academic year among student (aged 19 - 25 years) attending the University of Banja Luka the mean estimated daily sodium intake was 3,349mg. Processed meat products, fast food and bread and bakery products were the food groups that contributed the most to the total sodium intake [12]. Identifying sodium-potassium ratio in different population is important to establish health promoting policy. The objective of this study was to determine the content of sodium and potassium within the three-day meals at students of Faculty of Medicine.
Materials and Methods
A cross-sectional study covered 44 students at Faculty of Medicine of Sarajevo University. Before the study
students were introduced in the CINDI dietary guide [13], and became familiar with diet analysis software.
Exclusion criteria was health issues covered by medications. Students were divided into two group to estimate
sodium - potassium ratio in two seasons: winter and spring. The survey was conducted for the first group of
20 students during December of 2015 (4th, 5th and 6th December) and for the second group of 24 students
during April of 2016 (27th, 28th and 29th April).
The study was conducted according to the research ethics guidelines laid down in the Declaration of Helsinki [14]. Verbal informed consent was obtained from all students.
The research instrument was a self-administered questionnaire, which consisted of two parts. In the first
part of the survey, questions were related to age, sex, weight, height. The second part of the survey referred to
food frequency questionnaire (FFQ), as well as 3-Day Diet Record [15]. A record of all foods and beverages
consumed over a three-day period (consecutive days) included detailed information about each meal such
as the type and the amount of food and beverage. For dishes containing a combination of several different
food items, an amount for each component was recorded, such as condiments (mayonnaise, ketchup, gravy,
salad dressing, etc.). Individual foods and their quantities contained in the three-day meal were entered into
a computer program (free version of Nutritics Professional Nutrition Analysis Software) which provided
information of single nutrient intake.
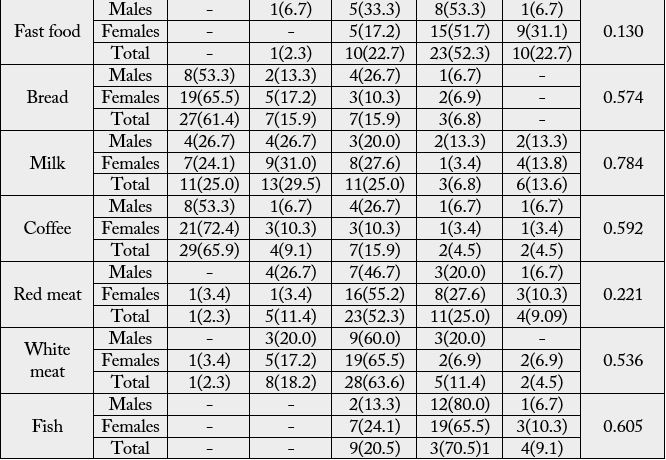
FFQ was formed according to dietary habits in our sample. The 15 items in the FFQ were fruits, raw vegetables, cooked vegetables, coca cola and beverages, sweets (ice cream, chocolate,…), cakes, chips, fried potatoes, fast food (hamburger, hotdog, sausages), bread and derivatives, milk, coffee, red meat, white meat, fish. There were five possible answers according to the frequency of consumption: (1) several times per day, (2) at least one time per day, (3) twice to three times per week, (4) twice to three times per month, and (5) never.
Registration of data was performed using the computer application Microsoft Excel 2013, while the analysis
of data was made using the Statistical Package for Social Sciences (version 13.0, SPSS, Inc) software. Results
were expressed as percentages and means±standard deviations. The chi square test was used to determine the
significance of categorical variables, while the significance of the difference for the continuous variables was
tested by the student t test for small independent samples. In the bivariate analysis, the association of sodium
and potassium intakes were estimated according to energy value of daily meal. Differences were considered
statistically significant at P < 0.05.
Results
A sample included a total of 44 students, of which: 15 (34.09%) were male and 29 (65.91%) were female.
The mean age of students participated in the study was 26.55±3.53 year. The mean weight was 74.64 ± 15.80
and mean height was 174.34 ± 9.36. Mean BMI was 24.33 ± 3.37. General information is shown in Table 1.
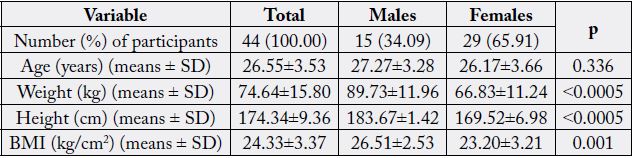
There were significant gender differences in relation to weight, height and BMI.
The analysis of the frequency of food consumed revealed that on daily level fruits were consumed by 24 (54.5%) students, raw vegetables by 16 (36.3%) students, sweets by 22 (50.0%) students. At 23 (52.3%) students fast food was part of daily meal twice to three times per month (Table 2).
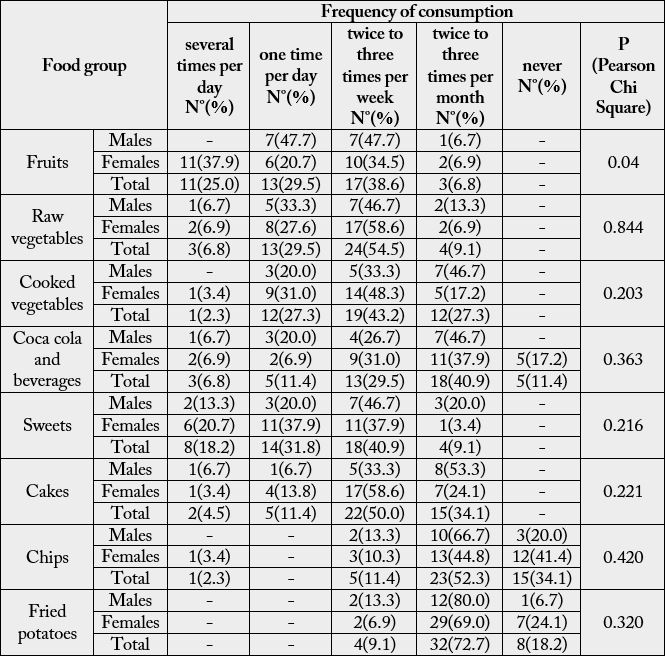
There was no statistic significant difference in frequency of food consumption between two student groups that took part in study in winter 2015 and spring 2016.
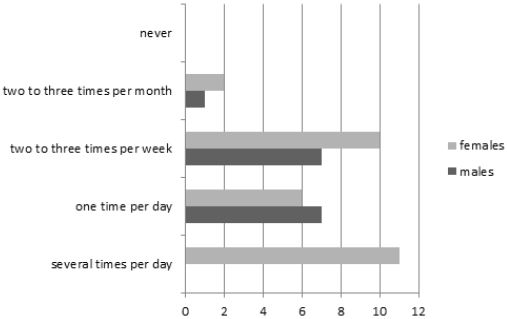
The pattern of consumption of fruits differed between gender (P=0.04). Female declared more frequent fruits consumption (Graph 1).
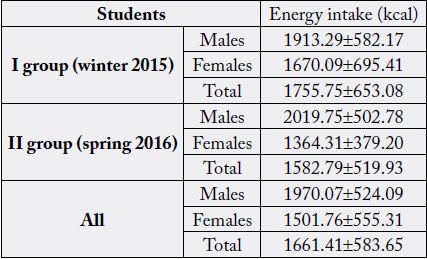
Within the three-day meal, the average energy intake was 1970.07±524.09 at males, and 1501.76±555.31 at females (Table 3).
Within the three-day meal, the average sodium intake was 1822.21±782.59mg, and the average potassium intake was 2443.55±651.48 as it is shown in Table 4.
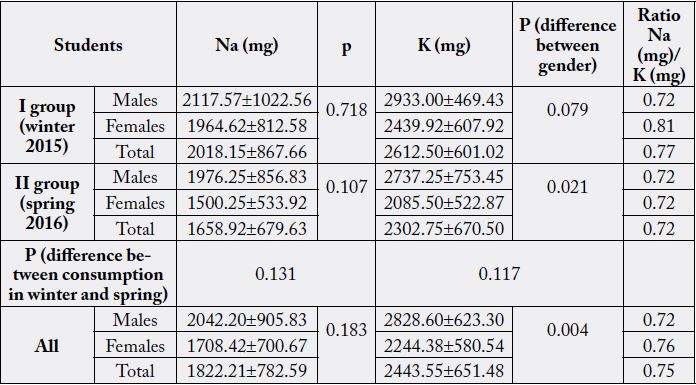
There was no statistically significant difference in the content of sodium or potassium in the winter and spring meals consumed over period of 3 days. However, a statistically significant difference in potassium content in the three-day meals was found between gender (P= 0.004).
Dietary sodium to potassium ratio was 0.75 in total sample.

** Correlation is significant at the 0.01 level
Discussion
Diet is a modifiable risk factor of a wide range of chronic diseases. Interventions in diet are related to
reduce risk for most endpoints [16]. Inadequate ratio between nutrients is global and action should be on
national level. Risk reduction strategies give longer lasting results among healthy young adults. Our study
was conducted in sample of students that were introduced in the CINDI dietary guide [13]. The objective of
this study was to determine the content of sodium and potassium within the three-day meals at students of
Faculty of Medicine. Between 12 key areas for action of the CINDI dietary guide, the recommendations on
vegetables and fruits intake and low-salt diet are the most important for potassium and sodium content of diet.
Through our results we tried to highlight the impact of adopted changes in dietary pattern on single nutrient
content. Average estimated sodium intake was 2042.20±905.83mg for males and 1500.25±533.92mg for
females. Average estimated potassium intake was 2828.60±623.30mg for males and 2244.38±580.54mg for
females. Average Na/K ratio of 0.72 for males, and 0.76 for females.
The 2020-2025 Dietary Guidelines for Americans emphasized that CDRR level for sodium is 2300mg/d, and AI for potassium is 2600mg/d for adult females (older than 19 years), and 3400mg/day for adult males (older than 19 years). According to these recommendations the normal range of dietary Na/K ratio is up 0.68 to 0.89 [17]. According to our results, no excess of sodium intake was found, and Na/K ratio was in recommended range. The strong correlation between sodium and potassium intakes with energy value of daily meal (P<0.01) did not disrupt this ratio.
There was no statistically significant difference in the content of sodium or potassium in the winter and spring meals consumed over period of 3 days. However, a statistically significant difference in potassium content in the three-day meals was found between gender (P=0.004). In contrast, female declared more frequent fruits consumption with a statistically significant difference between gender (P=0.04). These results indicate that it is important for some nutrient intake to choose the most suitable source in adequate serving size.
In our study we used individual measurements (FFQ and 3-Day Diet Record) for group-level analysis. Our students, in period of study, expressed good dietary choices. Thus through education lifestyle choices that support health can be empowered. There is no country-specific policy related to nutrient contents in Bosnia and Herzegovina. Reducing the sodium content in the diet of general population is a challenge for the food industry [18]. The food handler should be aware of the amount of salt present in the food [19]. Mathematical models are useful tools that can help to plan diets with adequate nutrients content with respect to food cost [20,21].
There are several limitations of this study and because of them participants in our sample had to be inform about them to try to avoid them as they could. Some limitations are linked to self-reported food recall, which leaves a possibility of underreporting or overreporting of actual intakes. Further used software has not been fully adapted to the market of Bosnia and Herzegovina and the labeling of salt content in retail foods is not obligatory in Bosnia and Herzegovina. Some of these issues are complex and should be resolved to at the national level.
Conclusion
The present study compares information obtained by two methods - FFQ and dietary food recall. Results
emphasize that it is important to choose healthy food in order to achieve adequate nutrient intake, as well
as also to have appropriate servings of chosen food.
Conflict of Interests
The authors declare that they have no competing interests.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!