Biography
Interests
Naisberg, Y.
Freelance, Haifa, Israel
*Correspondence to: Dr. Naisberg, Y., Freelance, Haifa, Israel.
Copyright © 2021 Dr. Naisberg, Y. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Multi-electrode cranial electric stimulation (CES) with a new Biophysical Mind Technology
(BMT) is a method for both non-invasive diagnosis (using 500 Microampere, 10Hz frequency, for
10msec) and for migraine treatment (using exposure with 100kHz frequency, 1.0mA and 250msec)
introduced to scalp through each pair out of 276 EEG combinations of electrode montage in 10-
20 EEG applications. Such method and device objectively measure brain electrical bioimpedance
units (BEBU) and induced voltage units (IVU), while all other CES lacking them.
To evaluate the effectiveness and safety of BMT-CES in reducing migraine pain and the correlation
between the clinical response and both BEBU and IVU.
Sixty migraine patients were randomly allocated to either treatment group or sham group. They
received twice a week BMT-CES or Sham-CES procedures for eight weeks. Migraine severity was
assessed by visual analogue scale (VAS) and the Migraine Disability Assessment Scale (MIDAS).
The experimental group displayed (with an ongoing CES sessions) a decrease in VAS and MIDAS
scores versus sham CES. Correlations between BEBU and IVU and VAS and MIDAS were
observed at the endpoint in the BMT-CES group but not the sham-CES group. A significant
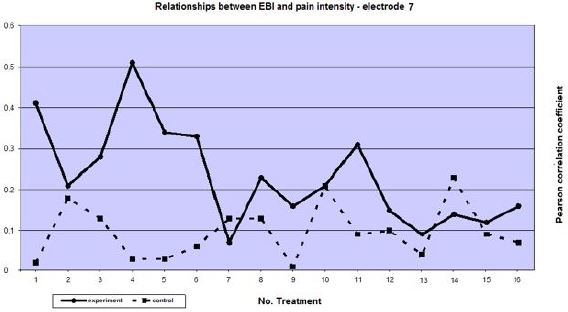
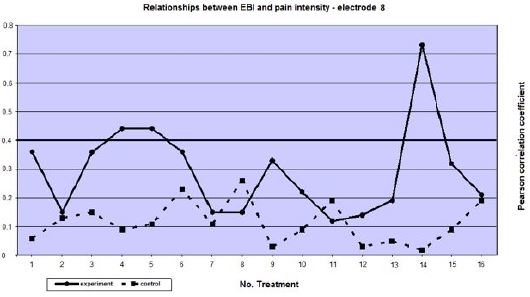
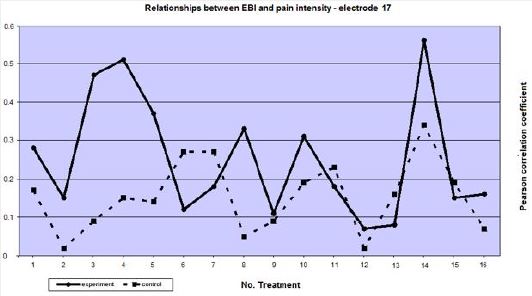
BEBU and IVU leveling indicate that electrodes 3, 7, 8 and 17 possess stable analgesic effects.
BMT-CES is a safe, non-invasive procedure to ameliorate migraine pain.
Introduction
Cortical spreading electrophysiological depression is implicated in the pathophysiology of migraine [1,2].
Mulleners et al [3,4] and Brighima et al [5] found visual cortical excitability in migraine. Aurora et al [6]
claimed that occipital cortex is hyper-excitable in migraine patients. In addition, Aurora [7] found that
cortical “silent” period is shortened in migraine patients.
Afra et al [8] showed influence of colors on habituation of visual evoked potentials in subjects suffering from migraine. In addition, Afra et al [9] detected inter-ictal cortical excitability also, at intervals between migraine attacks. Several authors [10-12] indicated on multiple factors participating in the pathogenesis of migraine, including ‘neurovascular contributors’ influencing perfusion, cerebral vascular reactivity, dysfunction in calcium channels, changes in blood CO2 levels and increased extracellular potassium.
Batteli et al [13] and Maertens de Noordhout [14] used TMS to reduce pain intensity in migraine patients. Solomon et al [15] used cranial electrotherapy to decrease migraine pain. Bystritsky et al [16] recently used CES procedure in treating anxiety disorders.
Our randomized, double-blind sham-controlled trial was designed to determine the safety and efficacy of multi-electrode cranial electric stimulation (CES) as a novel treatment modality for migraine symptoms, as well as the use of electrical bio-impedance values as a possible electromagnetic diagnostic tool in migraine. The primary goal of the CES treatment was to reduce the frequency, duration and pain intensity of migraine attacks, without intervening in their ongoing drug treatment. The secondary goal was to assess whether changed in non-invasive brain electrical bioimpedance units (BEBU) and induced voltage units (IVU) mapped on the head surface may be correlated with CES-related clinical improvement.
Methods
Population: Sixty migraine patients (17 men ,aged 42 to 64 years and 43women, aged 29 to 66 years) who
met the International Classification of Headache Diagnosis (ICDH) criteria for migraine [17] participated
in this study at four medical centers. They were recruited from a pool of migraine patients by neurological
teams. The patients suffered from migraine for at least 5 years and had at least one migraine attack per
week lasting for at least 30 hours per attack who did not respond to pharmacological treatments (>2 drugs).
Exclusion criteria were brain tumor, epilepsy, or transient ischemic attacks. All patients underwent pre-and
post -treatment EEG, clinical evaluation, blood count, as well as blood pressure monitoring at each session.
Migraine Disability Assessment Scale (MIDAS). The MIDAS evaluates the severity of the migraine by
a self-reporting scale that measures the subject’s daily functioning level. The MIDAS score system is :I.
Minimal or infrequent disability 0-5, II. Mild or infrequent disability 6-10, III. Moderate disability 11-20,
IV. Severe disability 21 + [18]. In addition, subjective clinical global impression of the intensity of headache
was assessed using visual analogue scale (VAS) of 10cm: 0 no pain at all, 10 maximal unbearable pain. Both
MIDAS and VAS were completed before each session. The trial was approved by the Bnei Zion Helsinki
committee and the Israeli Ministry of Health Helsinki Committee, and informed consent was obtained from
all participants after detailed oral and written explanation of the nature and procedures of the study. The 60
patients were randomly and blindly allocated to one of two groups (using computerized software): treatment
group (TG) underwent CES-based impendence assessment and afterwards CES treatment regimen, and
the control group (CG) underwent CES-based impendence assessment and afterwards sham CES. Both
patients and physicians were blind to the presence or absence of actual CES treatment. All patients were
asked to continue their regular nutrition, work, lifestyle and drug treatment. Fifty-eight patients completed
13-16 visits and were included in the final analysis. Thirty-three subjects received treatment with CES and
25 constituted the control group.
The CES device delivered identical multi-channel CES. The participants washed their head to ensure
appropriate electric conductance. Then, the electrodes were contacted to the head using a gym hat. The CES
or sham treatments were administered twice weekly.
Twenty-four electrodes were attached with a gel in a 10 to 20 EEG-like International Standardized System.
In such a way 24 electrodes cover the scalp all over the head. Each patient sat in front of a computer interface
engaged in a friendly topic. To achieve relaxation the interface showed a running rabbit from right to
left. After bioimpedance assessment for 69 seconds therapeutic CES was administered for 2 minutes. The
assessment phase included administration of 25kHz high frequency, 0.5mA and 10msec cycling time and
recording of bioimpedance and voltage-induced units in response to CES. Two and 4 weeks after termination
of 16 treatment or sham sessions, each participant underwent two impedance diagnostic procedures.
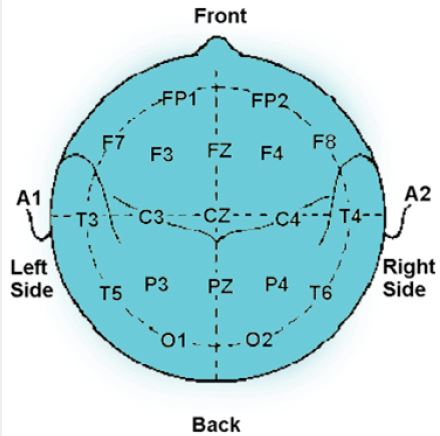
The impedance level between a pair of electrodes, attached to the skull area of each subject, was measured. 24 electrodes were connected to each subject, while creating a specific matrix structure of the electrodes. The impedance was measured between every pair of electrodes. A total of 276 measures (It is assumed that the impedance measured from electrode i to electrode i+1, for i=1,2,3, represents the impedance from (i+1) to i and therefore 276 is the total number of possible combinations), were obtained for each subject, accounting for combinations that cover nearly all areas of the brain (Fig.1).
For each subject, raw data were collected where each measure is registered for each pair of electrodes
separately. To allocate the impedance to each electrode, electrical bioimpedance (EBI), averaging was
performed for the impedance between each electrode to the 4-8 electrodes adjacent to it. This average represents
the impedance in the area surrounding the electrode. Electrodes 1 and 2 constituted reference points. The
average was calculated for the subjects in the two studied groups. Several steps were taken in order to best
represent the data. First for all raw data were tested every measurement, by registration data for each electrode
separately. Then the data were collected in both groups of patients when it became different for the electrical
bio-impedance averaging between each electrode to 4-8 electrodes that are nearby. Electrodes group position determined a priory with (electrodes 1 and 2 have been points of reference). The average composes the results
of subjects in both groups in each of the measurements made at 16 times that they came for treatment.
The treatment parameters of 100kHz of high frequency, 1.0mA and 250msec of cycling time were applied
through the 24 pairs of already attached electrodes. The sham group was exposed to the same electrodes
without CES administration. Whole treatment phase lasted about 10 minutes. CES or sham were
administered twice weekly for 8 weeks, total 16 treatments.
Two major approaches were used. The first operation is a two-factor variance analysis in mixed design
ANOVA to assess differences in the values of the electrical bioimpedance (EBI) and induced voltage (IV)
between pairs of electrodes in the matrices. The second analysis examined the subjective intensity of headache
(visual analog scale-VAS) and her/his daily functioning (MIDAS) during the time course of each subject
before each objective BEBU and IVU measurements, within each group and between the 2 study groups.
SPSS-15 software was used for statistical analysis.
Results
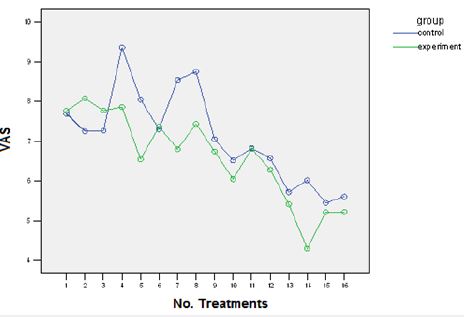
Figure 2 shows that the pattern of pain intensity measurements, as assessed by VAS, over time in the
experimental group is more pronounced than in the control group. The latter experience a significant
larger subjective reduction in the pain intensity than at baseline (p<0.005) compared with the subjects in
the control group. The subjective pain intensity in the experimental group decreased persistently with a
significant difference at the endpoint (p<0.01) in comparison to controls.
The measured difference in the MIDAS index, indicating the impairment in daily functioning during the period of three months, is depicted in Fig. 3.
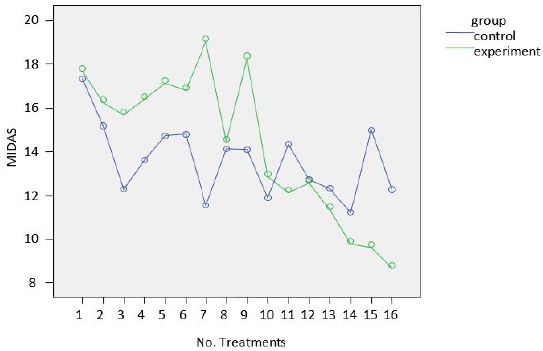
As shown in Figures 3 after the eleventh CES treatment there is a significant decline in the MIDAS scores with clearly significant difference (p <0.03) compared to the control group (sham CES) that continues throughout treatment , indicating gradual improvement in the daily functioning following the CES.
Response to treatment was considered when migraine-related disability reduced from stage III and IV (Moderate disability with 11-20 by MIDAS score) to stage II (Mild or infrequent disability with 6 - 10 MIDAS Scores).
Two analyses were applied: the first analysis is an inter-subject bi-factor variance analysis type Mixed Design designated to evaluate the differences in the impedance values, the induced current between the pair of the parallel electrodes in the matrix structure. The second analysis scan the intensity of headache and the functioning ability which the subject sensed during each one of the measures within each group separately and between the two study groups.
An interesting finding emerging from this analysis demonstrates that there are differences in the subject’s sensation pattern regarding the intensity level of his headache upon arriving at the lab between the different periods of time and between the two study groups. Figure 2 demonstrates that the pain intensity pattern, as assessed by the criterion of perception of headache intensity. As shown, in the control group along the measures the perception of headache intensity was more moderate than the pattern in the experiment group, while towards the last measures the subjects of the experiment group sense a significantly lower headache intensity than at the beginning of the experiment (p<0.005) as well as compared to the subjects in the control group (p<0.01).
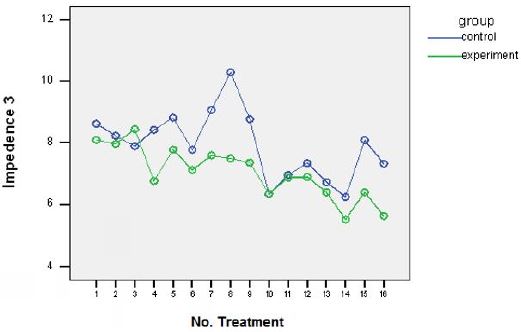
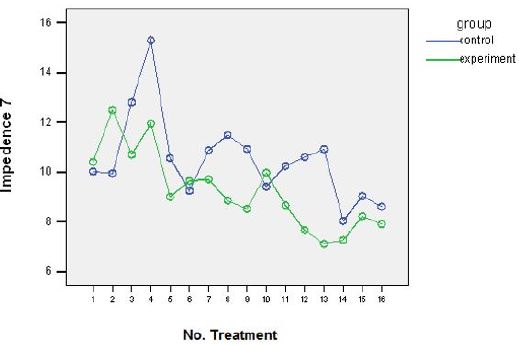
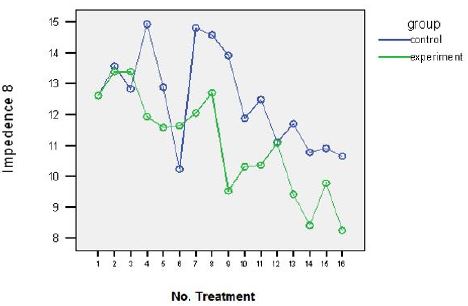
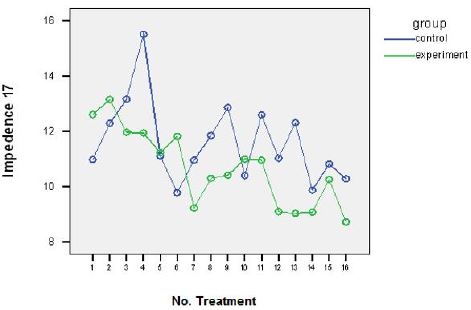
Apart from subjective measures of headache intensity perception and daily function the BEBU levels were examined at each visit in average across subjects in each of the 24 electrodes (with electrodes that are in its vicinity). By analyzing the decline in BEBU levels in the experimental group there was a significant correlation between the improvement in VAS and the reductions in the bioimpedance levels in 4 electrodes at the endpoint (number 3,7,8,17) (See Appendix 3).
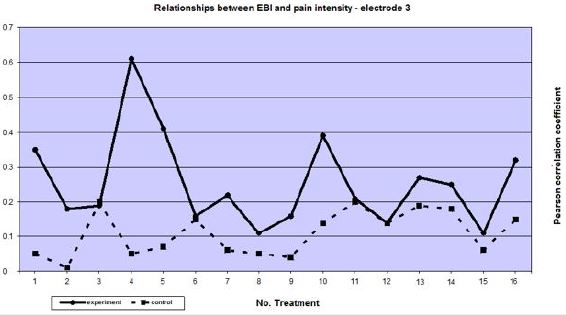
Also there are calculated BEBU relationships between headache intensity and laboratory electrodes reaching beyond sixteen specific measurements in the experimental and control groups. Table 1 shows the relationships electrodes which reduces BEBU during treatment over time of the number of measurements.

One can see in the experimental group there are significant positive relationships beyond the number of measurements. The BEBU levels with lower headache intensity. In the control group were not found such significant relationships.
Created in-depth analysis of these relationships in electrodes of a significant change seems to decrease in intensity of BEBU between patients who arrived with correspondent pain subjectivity confirmed by each BEBU measurement. In the experimental group throughout all measurements were positive relationships which strengthened between the two indices, so the BEBU level dropped down with a drop in the headache intensity whereas the control group did not change the intensity of these relationships and contacts throughout the measurements were not significant (see Appendix 4).
These findings allow the authors of the research to strengthen their hypothesis of being able with BEBU technology to find and target specific localizations on the scalp surface indicating on by leveling the BEBU beneath these brain regions one can control pain intensity reduction.
The treatment was associated with a decrease in the values of EBI under certain electrodes as opposed to other localized electrodes the headache intensity did not significantly differed. This finding presents the possibility to diagnose areas of the brain responsible for creating migraines providing a treatment tool the efficacy of which could be diagnosed with localized BEBU units. This represents a evidence for a combined objective tool for diagnosing and treating targeted scalp regions to alleviate or eliminate migraine attacks.
By identifying correct target scalp regions it would be possible to predict which BEBU levels may provoke a new migraine attack and monitoring their prevention.
These findings were reinforced by measuring induced voltage units (IVU) differences between pairs of electrodes that make up the structure of the matrices of the same placed electrodes. IVU differences were more significant during repeated measurements among specific pairs of electrodes likewise for localized BEBU. IVU were smaller in the experimental versus control group (p <0.01).
Discussion
In the present study we used a specialized Brain Mind Technology (BMT) apparatus that enabled to apply
safe multi-channel cranial electrotherapy stimulation (CES) and EEG electrodes to measure BEBU and
IVU at all treatment sessions. This approach was not used previously in CES devices (15,16). The BMTCES
was demonstrated to be able to monitor the electrical cortical spreading depression (1, 6) and visual
cortical hyper-excitability [3,4] in migraine patients. In particular, BMT-CES enabled to measure of BEBU
and IVU with 24 EEG electrodes in 276 stimulated pair combinations all over the scalp.
One of the advantages of the present study is that in addition to subjective measures of headache intensity awareness and daily function ( VAS and MIDAS) the BEBU levels were also examined at each visit using average within subjects in each of the 24 electrodes (with electrodes that are in its vicinity). By analyzing the decline in BEBU levels in the experimental group there was a significant correlation between the improvement in VAS and the reductions in the bioimpedance levels in 4 electrodes at the endpoint (number 3, 7, 8, 17. see Appendix 3) in the experimental group, but not in the sham group.
Thus, it appears that the headache intensity declined in parallel with a drop in the BEBU level in the BMT-CES group, whereas no such beneficial effect and correlation were achieved by the sham-CES (see Appendix 4).
These findings allow using the BEBU technology for identifying the target specific localizations on the scalp surface indicated by leveling the BEBU relevant for the pain intensity reduction. By identifying therapeutic relevant target scalp regions, it may be possible to predict which BEBU levels may provoke a new migraine attack and monitoring their prevention.
These findings were reinforced by measuring induced voltage units (IVU) differences between pairs of electrodes that make up the structure of the matrices of the same placed electrodes. IV differences were more significant during repeated measurements among specific pairs of electrodes.
A continuous change in impedance in four electrodes was detected during the course of treatment in association with a parallel clinical improvement only in the BMT-CES group. Further analysis of the relationship between the electrodes, in which the impedance decreased significantly and the migraine pain intensity merits further investigation. It is possible that these brain areas play a role in generating the migraine and are affected by electrical stimulation more than other areas, and therefore may be used for the diagnosis and treatment. It is of note that despite the low variance in the pain intensity, positive significant correlations were found between the clinical intensity of the headache and the degree of the impedance measured in the specific electrodes (3, 7, 8 and 17).
Conclusion
Significant correlations were found between objective electro- physiological measurements such as DEBU
and IVU in specific electrodes in correlation with subjective experience of relief in migraine pain intensity
and daily function in BMT-CES treated patients. These findings may enable optimal treatment with CES
apparatus that stimulates only relevant scalp areas (electrodes 3, 7, 8 and 17). Additional time-course studies
are needed for the identification of the minimal sessions needed to achieve a stable pain relief in migraine
patients and prevention of repeated migraine attacks.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!