Biography
Interests
Yasser Mohammed Hassanain Elsayed
Critical Care Unit, Fraskour Central Hospital, Damietta Health Affairs, Egyptian Ministry of Health (MOH), Damietta, Egypt
*Correspondence to: Dr. Yasser Mohammed Hassanain Elsayed, Critical Care Unit, Fraskour Central Hospital, Damietta Health Affairs, Egyptian Ministry of Health (MOH), Damietta, Egypt.
Copyright © 2021 Dr. Yasser Mohammed Hassanain Elsayed. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Hypocalcemia is a famous serious electrolyte disorder characterized by calcium deficiency. It is
recently associated with specific electrocardiographic changes such as both wavy triple and double
electrocardiographic signs (Yasser signs).
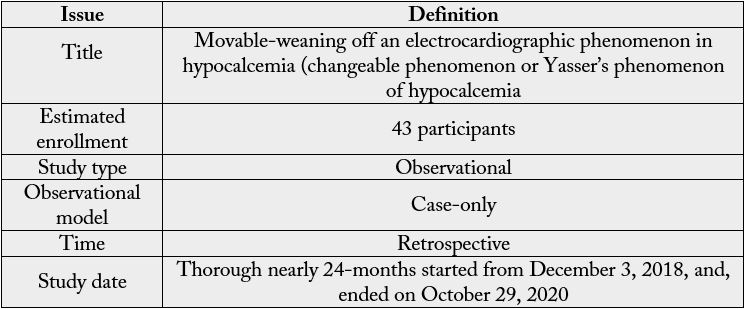
The study was observational and retrospective for 43 cases. The study was carried out at Fraskour
central hospital and the physician outpatient clinic. The author reported the 43-cases thorough
nearly 24-months, started from December 3, 2018, and, ended on October 29, 2020. Wavy triple
sign or Yasser sign of hypocalcemia was the target. Manifested or latent tetanies were fundamental
cases. Intravenous and oral calcium was used.
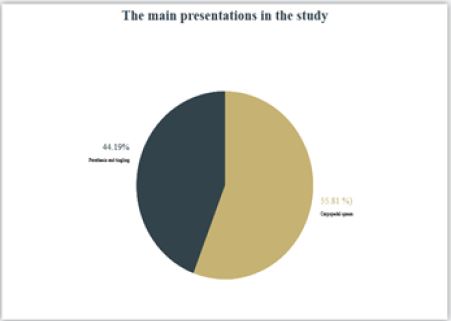
The age Mean was: 36.4 years, with the dominant female sex (67.44%). The main presentations in
the study were carpopedal spasm (55.81%) vs. Parathesia and tingling (44.19%). Hyperventilation
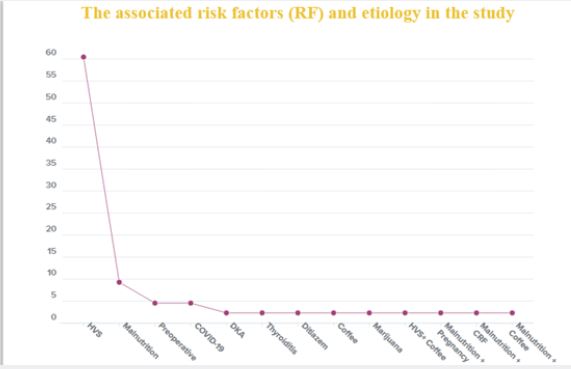
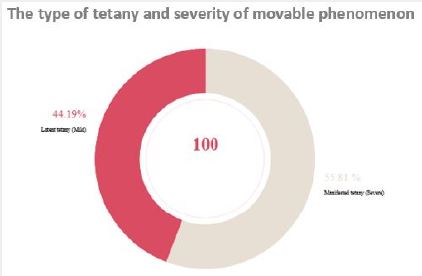
syndrome (60.47%) and malnutrition (9.3%) are the most frequent risk factors. Manifested tetany
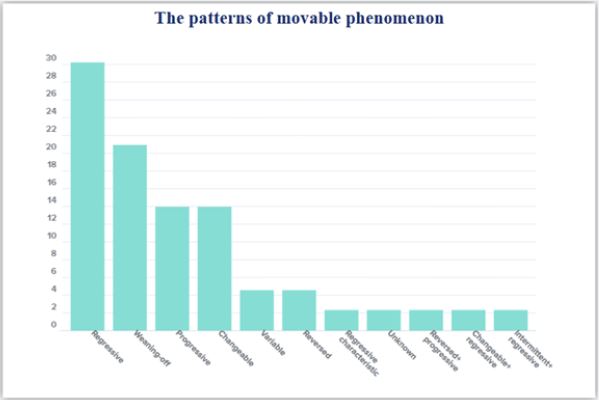
was the most common diagnosis (55.81). The patterns of Movable phenomenon were: regressive
(30.23%), weaning-off (20.93%), progressive (13.95%), changeable (13.95%), variable: 4.56%,
reversed (4.56%), regressive characteristic (2.33%), unknown (2.33%), reversed with progression
(2.33%) changeable with regression, (2.33%), and intermittent with regression (2.33%).
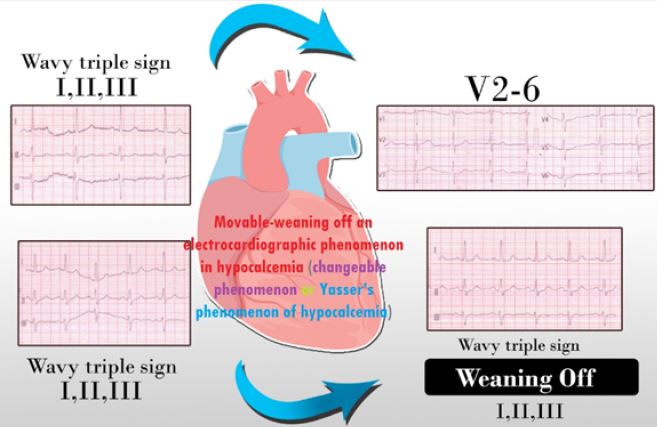
Movable-weaning off an electrocardiographic phenomenon in hypocalcemia (changeable
phenomenon or Yasser’s phenomenon of hypocalcemia) is defined according to the author’s opinion
in the study as a novel electrocardiographic phenomenon characterized by serial dynamic changes
in present in all cases of either Wavy triple or double electrocardiographic signs (Yasser signs) of
hypocalcemia. Movable-weaning off an electrocardiographic phenomenon is a guide for both Wavy
triple or double electrocardiographic signs (Yasser signs) of hypocalcemia. Don’t angry if the staring
electrocardiography or the last one was normal.
Abbreviations
ABG: Arterial blood gases
Ca++: Calcium
ECG: Electrocardiographic
ED: Emergency Department
IC: Intracellular
ICU: Intensive care unit
IV; IV: Intravenous
HF: Heart failure
POC: Physician outpatient clinic
RBS: Random blood sugar
SR: Sarcoplasmic reticulum
Introduction
The term of the latent type was elicited in the medical research in 1945 [1,2]. Hypocalcemia is a common
biological and clinical disease. It is a more broad variable in severity; starting from being asymptomatic
presentation in the mild cases extending to an acute fatal crisis in the most severe cases [3,4].
Calcium (Ca++) plays a vital structural role in the integration of myocardial function, cardiac output, and
vascular tone [5]. Calcium carries essential in the cellular mechanisms of myocardial contraction [3,6].
Calcium is a vital ion in many biochemical cycles such as cardiac automaticity; excitation with contraction
coupling in myocardial, smooth, and skeletal muscle; blood coagulation; neural conductivity; synaptic
propagation; hormone production, and mitosis. Calcium is considered the main intracellular (IC) messenger
needed for standard cellular activity and several enzymatic fuctions [7]. Calcium posses a pivotal effect in
tissues and organ injury in cases of ischemia, hypoxia, reperfusion, and toxic cell death [5]. Contraction of
smooth-muscles is linked to vibration in the IC Ca++ level [7]. Serum Ca++ level is commonly organized
within a narrow range (2.1 to 2.6mmol/L). Parathyroid hormone (PTH), vitamin D, and calcitonin are
considered calcium-regulating hormones. These metabolic pathways essentially occur in the bowel, kidneys,
and skeleton [8,9]. Approximately half of the total serum Ca++ is protein-bound but and the remaining half
is free ionized calcium which is physiologically active [9]. So, serum calcium levels are usually corrected on
consideration of the albumin level [8].
The ionized Ca++ is the vital physiological component that essentially indicates tight monitoring to assess
physiologically active calcium levels [5]. Total Ca++ in serum is ranged from 8.8 to 10.4mg/dl. Free ions,
Ca++ bound to albumin, and diffusible complexes are the main components. The concentration of free
calcium ions (4.8mg/dl) commonly affects several cellular processes. It is under closed hormonal control,
especially via PTH. In a patient with hypocalcemia, the serum albumin is necessary for the assessment of
actual hypocalcemia in the opposite of “factitious” hypocalcemia which is only associated with decreased
the total Ca++ [10]. Ionized Ca++ posses a critical function in organizing myocardial contractility. On the
occurrence of the cardiac action potential, ionized Ca++ enter IC via depolarization exciting Ca++ channels.
An IC ionized Ca++ activates calcium output from the sarcoplasmic reticulum (SR). Calcium combined
with the myofilaments proteins molecules especially, troponin C which is a trigger for the contraction of
myocardium [6,11]. The plasma ionized Ca++ concentration is preferably maintained in a narrow range (1.0
± 1.25mmol). This is happening despite a wide variation in the intestine and bony Ca++ input. Maintenance
of this range is essentially achieved by the action of three calciotropic hormones: parathyroid hormone,
calcitriol, and calcitonin [7]. Lethal hypocalcemic consequences commonly happen if the serum ionized
Ca++ concentration diminishes to below 2mg/d [7]. A bad prognosis was frequently recorded with ionized
hypocalcemia [5]. A significant improvement in cardiac output was observed after calcium administration
in the patients of severe ionized hypocalcemia (>30% decrease) [5].
Hypoparathyroidism, vitamin D, and albumin deficiency are the most common involved causes of
hypocalcemia [4,12]. Others causes include: End-stage renal disease or end-stage hepatic disease, pseudo
hypoparathyroidism or pseudopseudo hypoparathyroidism, metastatic or heavy metals e.g., CU++ and Fe++,
parathyroid gland carcinoma, eating disorders, magnesium changes, sclerotic bony metastases, hungry bone
syndrome, after parathyroidectomy, phosphate IV infusion, citrated massive blood transfusions, severe critical disorders, Fanconi syndrome, after exposure of parathyroid glands to radiation, renal failure, pancreatitis, calcium antagonists toxicity, rhabdomyolysis, tumor lysis syndrome, nutritional deficiency [3,4,12,13], druginduced
such as cinacalcet [14], 5-fluorouracil (5-FU) with leucovorin [15], high-dose of IV zoledronic acid
[4,5,13,16], acid phenobarbital [17], phenytoin [17], denosumab [18], foscarnet [12], and Na+ phosphate
preparations [19,20]. Falsely decreasing levels of CA++ due to albumin deficiency should be excluded by
serial monitoring of ionized CA++ [7]. Decreasing levels of ionized CA++ commonly happens in sepsis,
pancreatitis, magnesium deficiency, post-massive transfusions, post-neck operations, post-cession of
cardiopulmonary bypass in cardiovascular surgery, and after starting of extracorporeal membrane oxygenation
(ECMO) [5]. The symptoms are usually consistent with the proportion and promptness of the diminish
in serum CA++ [7]. Respiratory alkalosis post-hyperventilation, decreasing of potassium, adrenaline, after
psychogenic stress, and decreasing of magnesium may cause the symptoms of hypocalcemia [10,21].
Hypocalcemia in an emergency setting may be causing severe symptoms indicating hospital admission
[4,6,8]. But, the cases of gradually developing hypocalcemia are mostly will be asymptomatic [4,6,8].
Severe and acute hypocalcemia may be associated with Chvostek and Trousseau’s sign [6]. Broad- spectrum
of hypocalcemic signs and symptoms were recorded. It is including numbness, muscle spasms, cramps,
lassitude, weakness, tetany, circumoral numbness, fits, laryngospasm, bronchospasm, decreasing of blood
pressure, decreasing of heart rate, digitalis intolerance, tachycardia, heart failure (HF), sudden cardiac death,
hyperactive reflexes, neuromuscular irritability, cognitive deterioration, and personality disorders [4,7-
9,13,22]. The tingling sensation is the main presentation in hypocalcemia [6]. The diagnosis of latent tetany
is linked to the clinical signs accompanied by hypocalcemia in the presence of both Chvostek and Trousseau
signs. The expression “latent tetany” is quite mysterious [7]. Chvostek and Trousseau signs can be induced in
cases of hypocalcemia [4,13]. Diagnosis is usually confirmed with either corrected CA++ or ionized CA++
level [4].
Acute hypocalcemia is a predisposing factor for syncope, HF, and angina [23]. Calcium giving in cases of
severe ionized hypocalcemia (of >30% decrease) may be causing a marked amelioration in cardiac output
[5]. Calcium supplementation may correct a biochemical abnormality and thereby improve cardiovascular
status; in contrast, excessive calcium influx into the cells may contribute to cellular damage associated
with hypoxia [5]. An intense extracellular (EC) hypocalcemia corrupt myocardial contraction because the
SR can’t preserve enough quantity of Ca++ ion to start myocardial contraction [6]. The decreasing of cell
membrane potential is occurring in hypocalcemia. There is a rise in cell membrane permeability and cellular
muscle enzyme leakage [24]. Anyway, the increased cardiac enzymes are often restored to normal level
post-treatment of hypocalcemia [6]. Severe ionized hypocalcemia (≤40-50% of normal) is accompanied
by diminishing ventricular contractility, decreasing of heart rate, and dysfunction of vascular tone, and
hypotension [5].
Considering tobacco use as the target of interventions that facilitate the decrease of morbidity and mortality and augment quality of life in patients with hypertension and diabetes, this study’s aim was to evaluate smoking cessation in patients with hypertension and diabetes in general/family practice by applying the transtheoretical model.
The old non-specific ECG sign of hypocalcemia remains the QTc prolongation which is directly linked
to the grade of hypocalcemia and inversely linked to the serum Ca++ level [25]. Hypocalcemia is a wellestablished
cause of QT prolongation through the extension of the plateau phase of the cardiac action
potential [26,27]. Hypocalcemia causing QTc prolongation is a risk to serious ventricular arrhythmias [28].
Thus, it is causing Ca++ ion channels to be still open for a longer time, allowing a late Ca++ cellular inlet
and the generation of early after-depolarization [29,30]. If the threshold for depolarization is reached,
new action potentials are induced, initiating a tachycardia and re-entry. Torsades de pointes (TdP) and
ventricular fibrillation (VF) are serious arrhythmic complications of hypocalcemia [31]. QT prolongation
ST-intervals elongation, T-wave inversion, and decreasing heart rate are the ECG findings visible with
hypocalcemia [4,7]. The most common mechanisms of these ECG abnormalities are coronary artery spasm
[32]. Changes in the contour of the T-waves may be seen in all cases [26]. The U-wave is frequently absent
or unidentifiable [33]. Hypocalcemia may be inducing HF, elevation in cardiac enzymes, and ST-segment
alterations that simulate acute ST-segment elevation myocardial infarction (STEMI) [34]. Interestingly, the
patients may possess clinical and severe hypocalcemia without diagnostic ECG changes [33]. The physician
should understanding that the ECG may be normal during lethal hypocalcemia. So, normal ECG cannot
exclude this condition [7].
Wavy triple an Electrocardiographic Sign (Yasser Sign) is a new diagnostic sign originative in hypocalcemia. Wavy double an electrocardiographic sign also was reported in hypocalcemia that was commonly observed with either increasing or decreasing in the heart rate [35,36].
The analysis for this sign in the author interpretations are based on the following;
1. Different successive three beats in the same lead are affected.
2. All ECG leads can be implicated.
3. An associated elevated beat is visible with the 1st of the successive 3 beats, a depressing beat with the 2nd
beat, and isoelectric ST-segment in the 3rd one.
4. The elevated beat is either accompanied by ST-segment elevation or just a rising beat above the isoelectric
line.
5. Also, the depressed beat is either associated with ST-segment depression or just a depressing beat below
the isoelectric line.
6. The configuration for beat depressions, beat elevations, and isoelectricities of ST-segment for the successive
three beats are changeable from case to case. So, this arrangement non-conditional.
7. Mostly, there is no participation among the involved leads. The author suggested that the Wavy triple an
electrocardiographic sign not conditionally included in an especial coronary artery for the affected leads
[35].
An initial obtaining of electrolytes profile such as serum Ca++ levels serum, magnesium, phosphate levels with
arterial blood gas analysis, and albumin are essential workup to correctly diagnose and treat the underlying
electrolyte disorders. Calcium therapy should be immediately given without waiting for all laboratory results
especially if there are fits, asthmatic presentation, laryngospasm, and cardiac arrhythmias [10]. The ECG is
a helping diagnostic tool. Plain radiography or computed tomography (CT) scans are sometimes supportive
in the cases of rickets and osteomalacia [12]. Ionized Ca++ is the choice way for diagnosing hypocalcemia.
A serum Ca++ level less than 8.5mg/dL or an ionized Ca++ level less than 1.0mmol/L is true hypocalcemia
[12].
Delayed in the identification of the cause and treatment of hypocalcemic emergencies can lead to remarkably
in both morbidity or death [37]. Ionized hypocalcemia is commonly detected in critically-ill patients5. The
poorer prognosis is seen in the cases of ionized hypocalcemia [5].
It is important to note that hypomagnesemia may present with the same constellation of symptoms and
signs. So, preferably, serum Mg++ levels must also be monitor in all symptomatic patients. The maintenance
correction of hypocalcemia should be parallel with the management of hypomagnesemia [10]. Chronic
hypocalcemia is linked to either mild symptoms of neuromuscular irritability or quite asymptomatic [21].
Chvostek, Trousseau, and Erb sign are helping tests for elicit latent tetany [10]. Asssociated hypomagnesemia
should be considered in every patient of hypocalcemia [10,38]. Severe hypomagnesemia can be causing
resistant hypocalcemia for both calcium and vitamin D [12].
Management should be included in the patient’s symptoms and signs of hypocalcemia [10]. The treatment
of hypocalcemia is linked to the etiology, the degree, the existence of symptoms, and progression of
hypocalcemia developing [12]. Acute hypocalcemia is exceedingly mild and needs only supportive
management and additional workup monitoring [12]. Intravenous calcium is injected if serum Ca++ levels
decrease to below 1.9mmol/L, or ionized Ca++ levels are below than 1mmol/L, or if patients presented
without symptoms [4]. Hypocalcemic cases must be supported with oral calcium supplements and calcitriol
(0.25 to 1μg/day) as indicated [4]. Oral calcium, vitamin, and correction of hypomagnesemia should be
considered in management [10]. Calcium administraion may correct a biochemical defect with improving
cardiovascular effects. This happens in opposite of, excessive Ca++ cellular influx which may contribute to
cellular damage with hypoxia [5]. Calcium Supplementation in hypocalcemic cases may be accompanied by
hemodynamic amelioration [5]. Calcium injection to cases of severe ionized hypocalcemia (>30% decrease)
may be causing progress in cardiac output [5]. Correction of Ca++ deficiency maybe not adequate for the
restoration of myocardial function [6]. Serum ionized Ca++ is usually corrected within two weeks postcalcium
supplement [6]. Unfortunately, there is no approved precise formula for the assessment of serum Ca++ level in acute hypocalcemia [10]. Starting management of acute hypocalcemia with calcium should
be without waiting for the serum Ca++ levels [10]. Measuring of ionized Ca++ should be considered when
associated with acute or severe hypoalbuminemia [10].
The following formula [10] that can estimates the amount of Ca++ bound to protein: % protein-bound Ca = 8 (albumin, g/dl) + 2 (globulin, g/dl) + 3
Correction of hypoalbuminemia is used to determine the corrected serum Ca++ levels. The correction is to add 1mg/dl to the serum Ca++ level for each 1g/dl by which the albumin level is under 4g/dl [10]. Acute symptomatic hypocalcemia with serum Ca++ under 7.0mg/dl, and ionized Ca++ under 3.2mg/dl must be managed immediately with IV calcium [38]. Calcium gluconate is the drug of choice over calcium chloride. Calcium gluconate can be causing slight tissue necrosis if there are extravasations. The initial 100 to 200mg of elemental calcium (1-2 ampoules of 10% calcium gluconate [93mg/10ml ampoule]) must be given over 10-20 minutes. Calcium IVI should be diluted in 50 to 100ml of saline or dextrose solution to prevent any vein irritation [10]. Both calcium carbonate and calcium citrate possess the biggest amount of elemental calcium (40% and 28%, respectively). They are easily absorbed and the preferred supplements [22,39,40]. The standard doses of calcium supplement are ranging from1 to 2g of elemental calcium 3 times daily (level III evidence) [22]. Elemental calcium supplements can be initiated at 500 to 1000mg TDS with upward titration (level III evidence) [22]. All ECG abnormalities are often reversed post-calcium and calcitriol supplementation (level II evidence) [27]. IV calcium is given if serum Ca++ levels decrease below 1.9mmol/L, or ionized Ca++ levels are under than 1mmol/L, or if there are no symptoms (level III evidence) [8,9,41]. Prompt correction of calcium deficiency can be inducing cardiac arrhythmia [8,42]. Cardiac monitoring during IV calcium administration is vital, especially if the patient on digoxin medications (level III evidence) [8,22,43]. Chronic therapy fulfills persistent normalization of the ECG [44]. The clear improvements in the ECG abnormalities will be happening post-replacement of calcium and vitamin D [32].
Method of Study and Patients
My study was an observational retrospective for 43 cases. The study was done in Fraskour central hospital
and the physician outpatient clinic (POC). The author reported the 43-cases thorough nearly 24-months,
started from December 3, 2018, and, ended on October 29, 2020. Wavy triple an electrocardiographic
sign (Yasser Sign) of hypocalcemia was the target. Manifested or latent tetanies were fundamental cases.
Intravenous and oral calcium was used. (Table 1).
All the above criteria were assessed in parallel to the clinical status.
1. ECG artifact.
2. Ischemic heart disease and myocardial infarction
Case Presentations
The study was observational and retrospective for 43 cases. The study was carried out at Fraskour central
hospital and the physician outpatient clinic. The author reported the 43-cases thorough nearly 24-months,
started from December 3, 2018, and, ended on October 29, 2020. Manifested or latent tetanies were
fundamental cases. Most cases had been investigated for hypocalcemia that was undergoing serial ECG copies. Some cases were missed in investigations during the study due to many causes. ECG tracings were done
before and after calcium supplementation. Most cases were follow up for total and ionized calcium, and other
electrolytes before and after calcium supplementation. Random blood sugar was done for all cases. Arterial
blood gases (ABG), troponin test, serum albumin, and echocardiography were done in elected cases. Some of
the cases were admitted to the internal ward. Few cases were admitted or present in the ICU. The remaining
cases were managed in POC with later follow up. The serial ECG tracings are compared and examined for
the new phenomenon-in hypocalcemia;
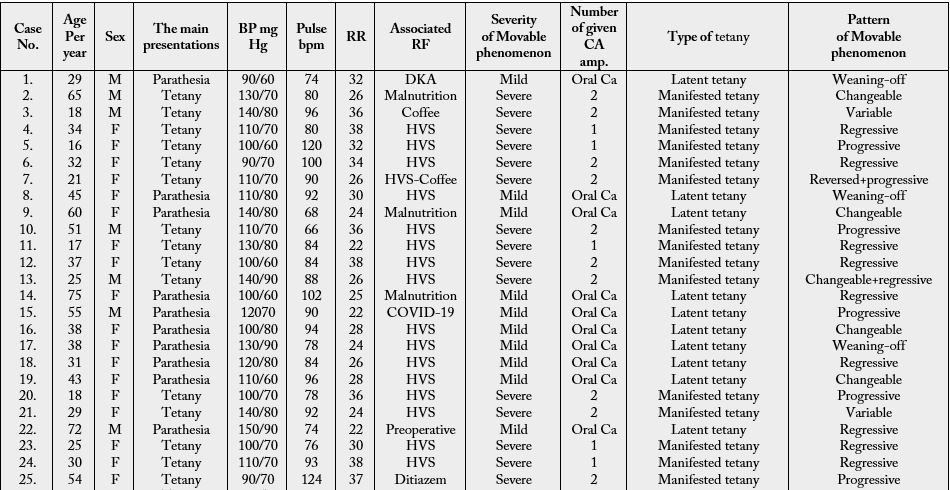
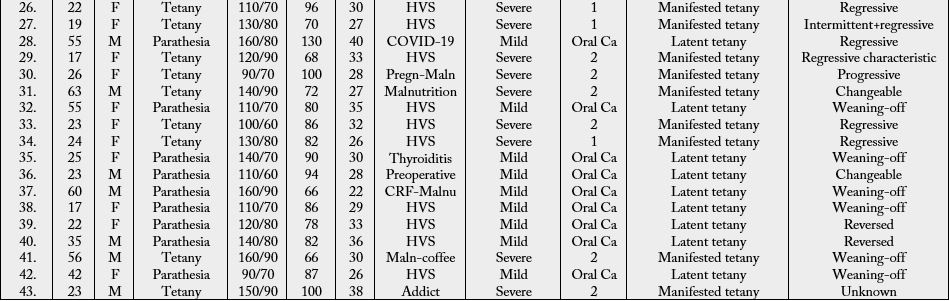
Addict**: Marijuana, BP: Blood Pressure, Ca: Calcium, DKA: Diabetic ketoacidosis, ECG: Electrocardiography, F: Female, HVS: Hyperventilation syndrome, M: Male, Malnut: Malnutrition, Pregn.: Pregnancy, RA: Risk factor, RR: Respiratory rate
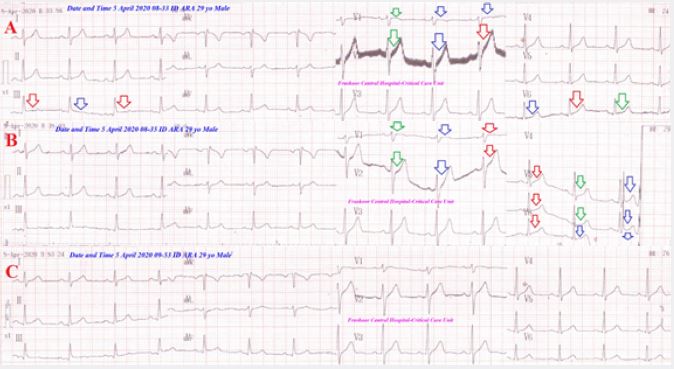
A 29-year-old married male carpenter Egyptian patient was admitted to the ICU due to diabetic ketoacidosis
and tachypnea. He was tested for latent tetany which was positive. Oral calcium-vitamin D tab was prescribed
for two weeks. Serial ECG tracings (A-C) showing an electrocardiographic wavy triple sign of hypocalcemia
and
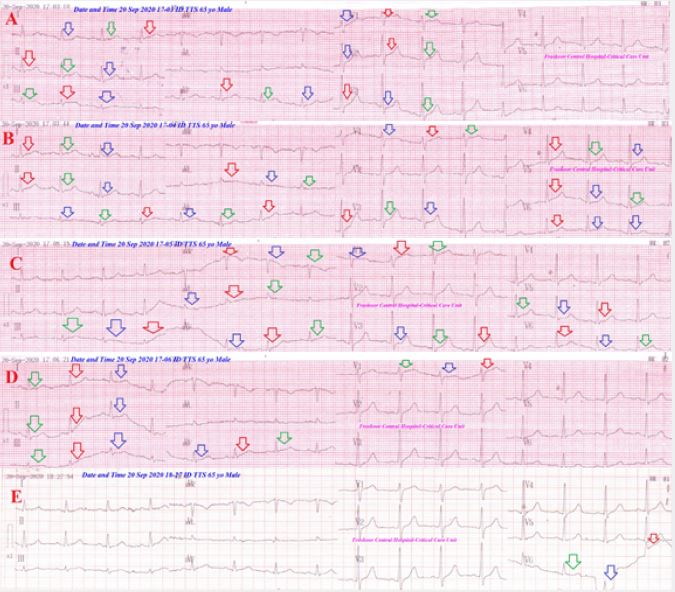
A 65-year-old married male carpenter Egyptian patient presented to the ED with hypoglycemia, tetany,
tachypnea, and chest pain. The patient had a long history of malnutrition due to poverty. Two-calcium
gluconate ampoules (10ml 10%) over IV over 20 minutes was given. Serial ECG tracings (A-E) showing an
electrocardiographic wavy triple sign of hypocalcemia and
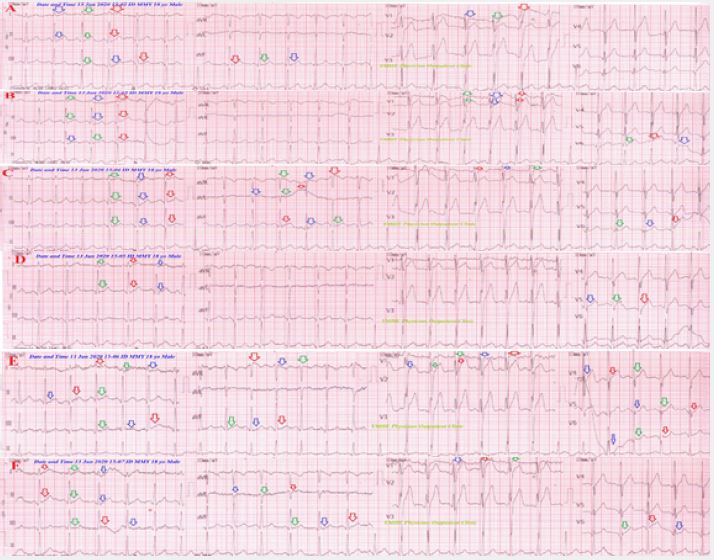
A 18-year-old single student male Egyptian patient presented to the POC with hyperventilation syndrome
and tetany. The relatives gave a long history of malnutrition and heavy coffee drinking. Two-calcium
gluconate ampoules (10ml 10%) over IV over 20 minutes was given. Serial ECG tracings (A-F) showing an electrocardiographic wavy triple sign of hypocalcemia and a Variable pattern of the movable phenomenon.
Clinical and ECG recovery had occurred (Figure 4).
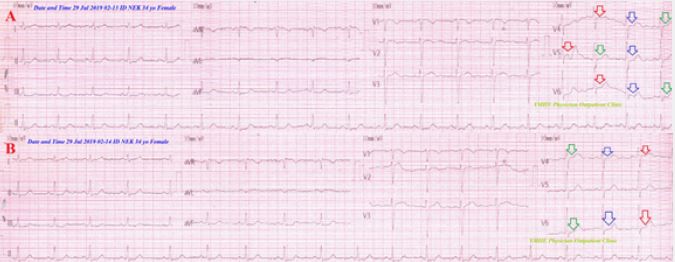
A 34-year-old married Egyptian housewife female patient presented to the POC with tetany and hyperventilation syndrome. The relatives gave a long history of malnutrition. One-calcium gluconate ampoule
(10ml 10%) over IV over 10 minutes was given. Serial ECG tracings (A-B) showing an electrocardiographic
wavy triple sign of hypocalcemia and
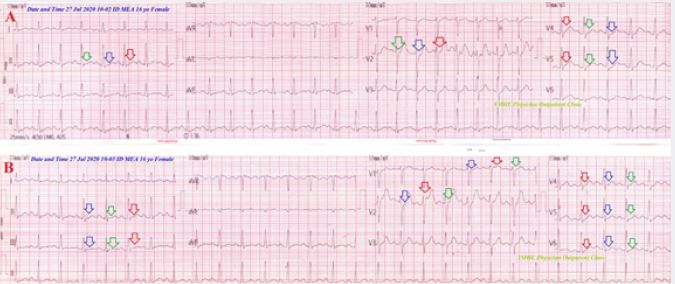
A 16-year-old single Egyptian student female patient presented to the POC with tetany and hyperventilation
syndrome. The patient gave a recent history of psychological troubles. one-calcium gluconate ampoule (10ml
10%) over IV over 10 minutes was given. Serial ECG tracings (A-B) showing an electrocardiographic wavy
triple sign of hypocalcemia and a
A 32-year-old married Egyptian housewife female patient presented to the ED with tetany and
hyperventilation syndrome after suicidal attempt with dextromethorphan HCL syrup. The patient gave
a recent history of psychological troubles. Two-calcium gluconate ampoules (10ml 10%) over IV over
20 minutes was given. Serial ECG tracings (A-B) showing an electrocardiographic wavy triple sign of
hypocalcemia and

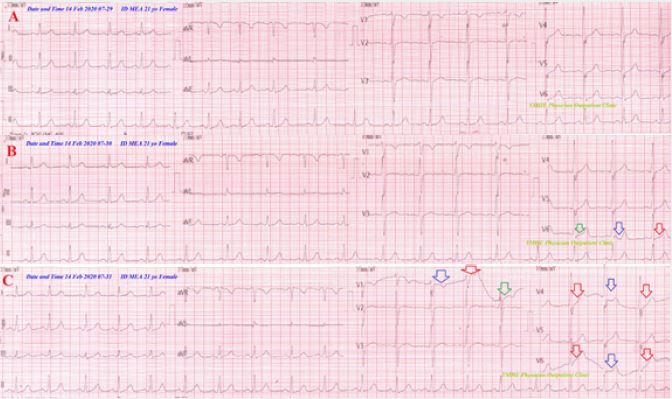
A 21-year-old single Egyptian student female patient presented to the POC with tetany and hyperventilation
syndrome. There was a recent history of psycho-familial troubles. She gave a history of heavy coffee drinking.
Two-calcium gluconate ampoules (10ml 10%) over IV over 20 minutes was given. Serial ECG tracings
(A-C) showing
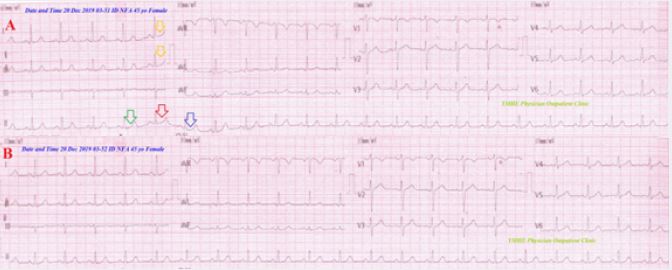
A 45-year-old married Egyptian female patient presented to the POC with hyperventilation syndrome.
There was a recent history of financial stress. He was tested for latent tetany which was positive. Oral
calcium-vitamin D tab was prescribed for two weeks. Serial ECG tracings (A-B) showing
A 60-year-old married Egyptian housewife female patient presented to the POC with tachypnea and
hyperventilation syndrome. The patient gave a history of poor nutritional status, hypertensive, and heart
failure. He was tested for latent tetany which was positive. Oral calcium-vitamin D tab was prescribed for
two weeks. Serial ECG tracings (A-B) showing an electrocardiographic wavy triple sign of hypocalcemia
and
A 51-year-old married Egyptian officer male patient presented to the ED with tetany and hyperventilation
syndrome. The patient gave a recent history of work psychological stress. Two-calcium gluconate ampoules
(10ml 10%) over IV over 20 minutes was given. Serial ECG tracings (A-C) showing an electrocardiographic
wavy triple sign of hypocalcemia and

A 17-year-old single, student, Egyptian female patient presented to the emergency department (ED) with
carpopedal spasm and hyperventilation syndrome. The patient gave a recent history of socio-familial stress.
One-calcium gluconate ampoule (10ml 10%) over IV over 10 minutes was taken. Serial ECG tracings
(A-C) showing an electrocardiographic wavy triple sign of hypocalcemia and
A 37-year-old married Egyptian housewife female patient presented to the ED with tetany, dizziness,
and hyperventilation syndrome. The patient gave a recent history of psycho-familial stress. Two-calcium
gluconate ampoules (10ml 10%) over IV over 20 minutes was given. Serial ECG tracings (A-B) showing an
electrocardiographic wavy triple sign of hypocalcemia and
A 25-year-old married Egyptian painter male patient presented to the POC with tetany and hyperventilation
syndrome. The patient gave a recent history of psychological stress. He is a heavy coffee drinker. Two-calcium
gluconate ampoules (10ml 10%) over IV over 20 minutes was given. Serial ECG tracings (A-B) showing
an electrocardiographic wavy triple sign of hypocalcemia and
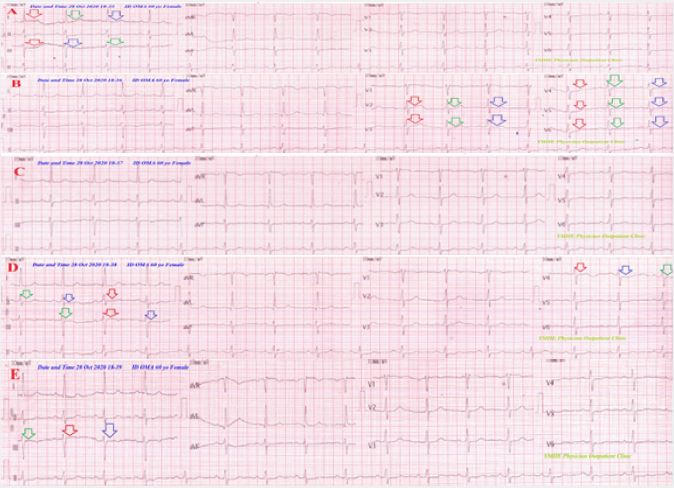
A 75-year-old married Egyptian housewife female patient presented to the POC with marked tachypnea
and palpitations. The patient gave a history of poor nutritional status, hypertensive crises, and heart failure.
He was tested for latent tetany which was positive. Oral calcium-vitamin D tab was prescribed for two
weeks. Serial ECG tracings (A-C) showing an electrocardiographic wavy triple sign of hypocalcemia and
A 55-year-old married Egyptian carpenter male patient presented to the POC with marked tachypnea
chest pain, and palpitations. The patient gave a recent history of COVID-19 with a history of hypertensive
crises. He was tested for latent tetany which was positive. Oral calcium-vitamin D tab was prescribed for
two weeks. Serial ECG tracings (A-C) showing an electrocardiographic wavy triple sign of hypocalcemia
and
A 38-year-old married Egyptian housewife female patient presented to the POC with tachypnea and
hyperventilation syndrome. The patient gave a recent history of psycho-familial stress. He was tested for
latent tetany which was positive. Oral calcium-vitamin D tab was prescribed for two weeks. Serial ECG
tracings (A-B) showing an electrocardiographic wavy triple sign of hypocalcemia and
A 38-year-old married Egyptian housewife female patient presented to the POC with tachypnea and
hyperventilation syndrome. The patient gave a recent history of psycho-familial stress. He was tested for
latent tetany which was positive. Oral calcium-vitamin D tab was prescribed for two weeks. Serial ECG
tracings (A-B) showing an electrocardiographic wavy triple sign of hypocalcemia and
A 31-year-old married Egyptian housewife female patient presented to the POC with tachypnea and
hyperventilation syndrome. The patient gave a recent history of psycho-familial stress. He was tested for
latent tetany which was positive. Oral calcium-vitamin D tab was prescribed for two weeks. Serial ECG
tracings (A-B) showing an electrocardiographic wavy triple sign of hypocalcemia and
A 43-year-old married Egyptian housewife female patient presented to the POC with tachypnea, tetany,
and psychogenic hemiplegia. The patient gave a recent history of psycho-familial stress. He was tested for latent tetany which was positive. Oral calcium-vitamin D tab was prescribed for two weeks. Serial ECG
tracings (A-B) showing an electrocardiographic wavy triple sign of hypocalcemia and
A 18-year-old single, student, Egyptian female patient presented to the emergency department (ED) with
carpopedal spasm and psychogenic hyperventilation syndrome. The patient gave a recent history of sociofamilial
stress. Two-calcium gluconate ampoules (10ml 10%) over IV over 20 minutes was given. Serial
ECG tracings (A-C) showing an electrocardiographic wavy triple sign of hypocalcemia and
A 29-year-old married, teacher, Egyptian female patient presented to the POC with carpopedal spasm
and psychogenic hyperventilation syndrome. The patient gave a recent history of socio-familial stress. Twocalcium
gluconate ampoules (10ml 10%) over IV over 20 minutes was given. Serial ECG tracings (A-C)
showing an electrocardiographic wavy triple sign of hypocalcemia and
A 72-year-old married, farmer, Egyptian male patient presented to POC with tachypnea. The patient present
for preoperative preparation for benign prostatic hypertrophy. He was tested for latent tetany which was
positive. Oral calcium-vitamin D tab was prescribed for two weeks. Serial ECG tracings (A-B) showing an
electrocardiographic wavy triple sign of hypocalcemia and
A 25-year-old married Egyptian housewife female patient presented to the POC with tachypnea and
hyperventilation syndrome. The patient gave a recent history of psycho-familial stress. One-calcium
gluconate ampoule (10ml 10%) over IV over 10 minutes was given. Serial ECG tracings (A-B) showing an
electrocardiographic wavy triple sign of hypocalcemia and
A 30-year-old married Egyptian housewife female patient presented to the POC with tachypnea and
hyperventilation syndrome. The patient gave a recent history of psycho-familial stress. One-calcium
gluconate ampoule (10ml 10%) over IV over 10 minutes was given. Serial ECG tracings (A-B) showing an
electrocardiographic wavy triple sign of hypocalcemia and
A 54-year-old married Egyptian housewife female patient presented to the ED with tetany, angina, and
hyperventilation syndrome. The patient gave a recent history of swallowing a heavy dose of oral diltiazem.
Two-calcium gluconate ampoules (10ml 10%) over IV over 20 minutes was given. Serial ECG tracings
(A-B) showing an electrocardiographic wavy triple sign of hypocalcemia and
A 22-year-old married Egyptian housewife female patient presented to the ED with tetany and
hyperventilation syndrome. The patient gave a recent history of psycho-familial stress. One-calcium
gluconate ampoule (10ml 10%) over IV over 10 minutes was taken. Serial ECG tracings (A-C) showing an
electrocardiographic wavy triple sign of hypocalcemia and
A 19-year-old single Egyptian student female patient presented to the POC with tetany and hyperventilation
syndrome. The patient gave a recent history of psychological stress. One-calcium gluconate ampoule (10ml
10%) over IV over 10 minutes was given. Serial ECG tracings (A-C) showing an electrocardiographic
wavy triple sign of hypocalcemia and
A 55-year-old married Egyptian carpenter male patient presented to the POC with severe tachypnea. The
patient was admitted to the ICU due to COVID-19 pneumonia. He was tested for latent tetany which was
positive. Oral calcium-vitamin D tab was prescribed for two weeks. Serial ECG tracings (A-B) showing an
electrocardiographic wavy triple sign of hypocalcemia and a Regressive pattern of the movable phenomenon.
Clinical and ECG recovery had occurred.
A 17-year-old single Egyptian student female patient presented to the ED with tetany and hyperventilation
syndrome. The patient gave a recent history of psychological stress. Two-calcium gluconate ampoules (10ml
10%) over IV over 20 minutes was taken. Serial ECG tracings (A-B) showing an electrocardiographic wavy
triple sign of hypocalcemia and a Regressive with
A 26-year-old married Egyptian housewife pregnant female patient presented to the POC with tetany and
hyperventilation syndrome. There is a long history of malnutrition. Two-calcium gluconate ampoules (10ml 10%) over IV over 20 minutes was given. Serial ECG tracings (A-B) showing a wavy triple sign of
hypocalcemia and
A 63-year-old married Egyptian fisherman male patient presented to the ED with tetany and hyperventilation
syndrome. There was a long history of malnutrition. Two-calcium gluconate ampoules (10ml 10%) over
IV over 20 minutes was given. Serial ECG tracings (A-B) showing both
A 55-year-old married housewife Egyptian female patient presented to the POC with hyperventilation
syndrome. There was a recent history of the socio-familial event. He was tested for latent tetany which was
positive. Oral calcium-vitamin D tab was prescribed for two weeks. Serial ECG tracings (A-B) showing
wavy triple sign of hypocalcemia with
A 23-year-old married housewife Egyptian female patient presented to the POC with hyperventilation
syndrome. There was a recent history of the socio-familial event. Two-calcium gluconate ampoules (10ml
10%) over IV over 20 minutes was taken. Serial ECG tracings (A-B) showing a wavy triple sign of
hypocalcemia with
A 24-year-old married housewife Egyptian female patient presented to the POC with tetany and
hyperventilation syndrome. There was a recent history of the socio-familial event. One-calcium gluconate
ampoule (10ml 10%) over IV over 10 minutes was given. Serial ECG tracings (A-C) showing wavy triple
sign of hypocalcemia with
A 25-year-old housewife, married, Egyptian female patient presented to the POC with tachypnea. The
patient gave a history of inflammatory thyroiditis with hypocalcemia. He was tested for latent tetany
which was positive. Oral calcium-vitamin D tab was prescribed for two weeks. Serial ECG tracings (A-B)
showing an electrocardiographic wavy triple sign of hypocalcemia and
A 23-year-old single student male Egyptian patient presented to the POC with hyperventilation syndrome.
The patient presented for preoperative preparation. He was tested for latent tetany which was positive.
Oral calcium-vitamin D tab was prescribed for two weeks. Serial ECG tracings (A-C) showing an
electrocardiographic wavy triple sign of hypocalcemia and a Changeable pattern of the movable phenomenon.
Clinical and ECG recovery had occurred.
A 60-year-old farmer, married, Egyptian male patient presented to ED with chest pain and tachypnea.
The patient gave a history of chronic renal impairment and malnutrition. He was tested for latent tetany
which was positive. Oral calcium-vitamin D tab was prescribed for two weeks. Serial ECG tracings (AB)
showing an electrocardiographic wavy triple sign of hypocalcemia and a Weaning-off pattern of the
movable phenomenon. Clinical and ECG recovery had occurred.
A 17-year-old single Egyptian student female patient presented to the POC with tachypnea and
hyperventilation syndrome. The patient gave a recent history of psycho-familial stress. He was tested for
latent tetany which was positive. Oral calcium-vitamin D tab was prescribed for two weeks. Serial ECG
tracings (A-B) showing an electrocardiographic wavy triple sign of hypocalcemia and a Weaning-off pattern
of the movable phenomenon. Clinical and ECG recovery had occurred.
A 22-year-old married Egyptian housewife female patient presented to the ED with tachypnea and
hyperventilation syndrome. The patient gave a recent history of psycho-familial stress. She was tested for
latent tetany which was positive. Oral calcium-vitamin D tab was prescribed for two weeks. Serial ECG
tracings (A-B) showing an electrocardiographic wavy triple sign of hypocalcemia and
A 35-year-old governmental officer, married, Egyptian male patient presented to POC with tachypnea.
The patient gave a recent history of psycho-familial stress. He was tested for latent tetany which was
positive. Oral calcium-vitamin D tab was prescribed for two weeks. Serial ECG tracings (A-B) showing an
electrocardiographic wavy triple sign of hypocalcemia and
A 56-year-old a married Egyptian farmer male patient presented to the POC with tetany, palpitations, and
hyperventilation syndrome. The patient gave a long history of malnutrition and heavy coffee drinking. Two- calcium gluconate ampoules (10ml 10%) over IV over 20 minutes was taken. Serial ECG tracings (AB)
showing an electrocardiographic wavy triple sign of hypocalcemia and
A 42-year-old married Egyptian housewife female patient presented to the POC with tachypnea and
hyperventilation syndrome. The patient gave a recent history of psycho-familial stress. He was tested for
latent tetany which was positive. Oral calcium-vitamin D tab was prescribed for two weeks. Serial ECG
tracings (A-B) showing an electrocardiographic wavy triple sign of hypocalcemia and
A 23-year-old single Egyptian Coffee-maker male patient presented to the ED with tetany and
hyperventilation syndrome. The patient gave a recent history of psychological stress. He is a marijuana abuse.
Two-calcium gluconate ampoules (10ml 10%) over IV over 20 minutes was given. Serial ECG tracings
(A-B) showing an electrocardiographic wavy triple sign of hypocalcemia and
Results and Findings
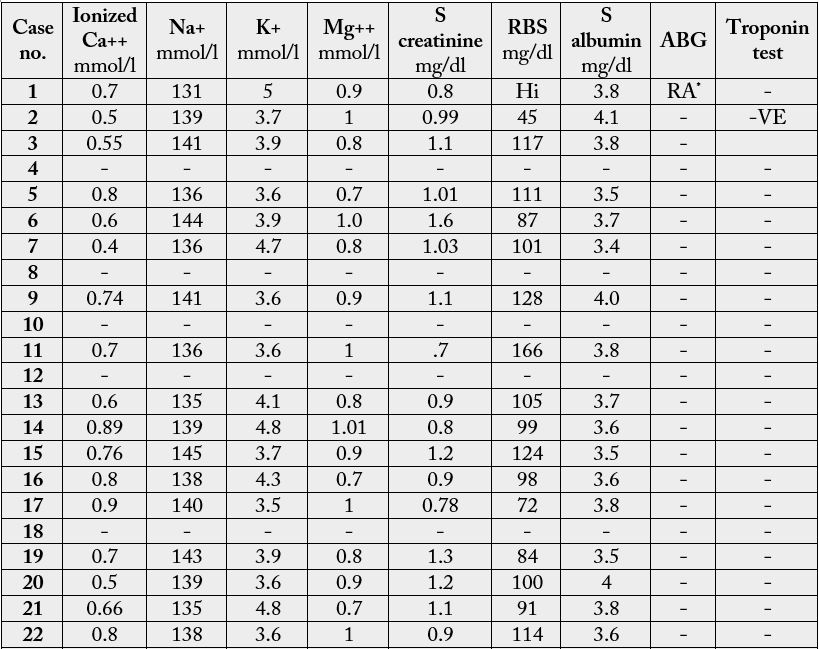
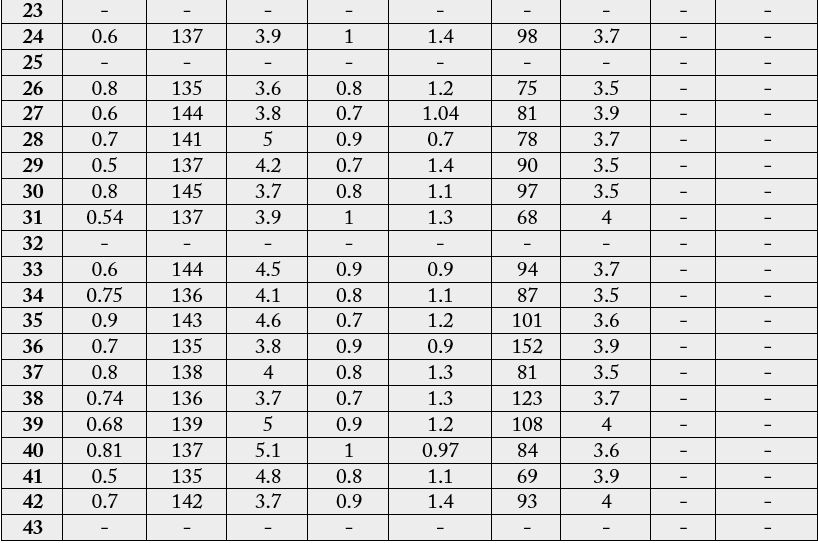
ABG: arterial blood gases, Ca++: calcium, Na+: sodium K+: potassium, Mg++: magnesium, RA: respiratory alkalosis, RBS: random blood sugar
• HVS: 60.47% (26 cases)
• Malnutrition: 9.3% (4 cases)
• Preoperative: 4.56% (2 cases)
• COVID-19: 4.56% (2 cases)
• DKA: 2.33% (1 case)
• Thyroiditis: 2.33% (1 case)
• Ditiazem : 2.33% (1 case)
• Coffee: 2.33% (1 case)
• Marijuana: 2.33% (1 case)
• Combined RF:
• HVS+ Coffee: 2.33% (1 case)
• Malnutrition + Pregnancy: 2.33% (1 case)
• Malnutrition + CRF: 2.33% (1 case)
• Malnutrition + Coffee: 2.33% (1 case) (Figure-13).
• Manifested tetany (Severe): 55.81% (24 cases)
• Latent tetany (Mild): 44.19% (19 cases) (Figure-14).
• Regressive: 30.23% (13 cases)
• Weaning-off: 20.93% (9 cases)
• Progressive: 13.95% (6 cases)
• Changeable: 13.95% (6 cases)
• Variable: 4.56% (2 cases)
• Reversed: 4.56% (2 cases)
• Regressive characteristic: 2.33% (1 case)
• Unknown: 2.33% (1 case)
• Reversed+ progressive: 2.33% (1 case)
• Changeable+ regressive : 2.33% (1 case)
• Intermittent+ regressive: 2.33% (1 case) (Figure-15).
Discussion
1. Movable-weaning off an electrocardiographic phenomenon in hypocalcemia (changeable phenomenon or
Yasser’s phenomenon of hypocalcemia) is defined according to the author’s opinion in the study as a novel
electrocardiographic phenomenon characterized by serial dynamic changes in either Wavy triple or double
electrocardiographic signs (Yasser signs) of hypocalcemia.
2. The dynamic changes either progression, regression, changeable, variable, weaning-off, or reversed.
3. The target was in the author’s opinion was the Wavy triple and double electrocardiographic signs (Yasser signs) which can be movable from lead to lead through the ECG of hypocalcemia.
4. Serial ECG tracings are an essential tool for understanding the new phenomenon and its verifications.
5. Movable-weaning off electrocardiographic phenomenon is a directory for the course of both Wavy triple or double an electrocardiographic signs (Yasser signs) of hypocalcemia.
6. The patients was secondly classified according to “Pattern of extension of Movable-weaning off an electrocardiographic phenomenon;
Conclusions
• Movable-weaning off an electrocardiographic phenomenon in hypocalcemia (changeable phenomenon or
Yasser’s phenomenon of hypocalcemia) is defined according to the author’s opinion in the study as a novel
electrocardiographic phenomenon characterized by serial dynamic changes in present in all cases of either
Wavy triple or double electrocardiographic signs (Yasser signs) of hypocalcemia.
• Movable-weaning off an electrocardiographic phenomenon is a guide for both Wavy triple or double electrocardiographic signs (Yasser signs) of hypocalcemia.
• Don’t angry if the staring electrocardiography tracing or the last one was normal.
• Further investigations for the “Movable-weaning off an electrocardiographic phenomenon in hypocalcemia (changeable phenomenon or Yasser’s phenomenon of hypocalcemia) for more evaluation and assessment are recommended.
Conflicts of Interests
There are no conflicts of interest.
Acknowledgment
I wish to thank Dr. Ameer Mekkawy; M.Sc. for technical support and nurses of the Critical Care Unit, and
Emergency Department who make extra-ECG copies for helping me.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!