Biography
Interests
Esmael Ali Hamed
Vascular and Endovascular Surgery Consultant, Mansoura New General Hospital (International) and Head of Vascular Surgery Department at Mansoura Health Insurance Hospital, Mansoura, Egypt
*Correspondence to: Dr. Esmael Ali Hamed, Vascular and Endovascular Surgery Consultant, Mansoura New General Hospital (International) and Head of Vascular Surgery Department at Mansoura Health Insurance Hospital, Mansoura, Egypt.
Copyright © 2020 Dr. Esmael Ali Hamed. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Functioning vascular access (VA) is our target to build an efficient hemodialysis procedure [1,2]. There are three main types of access: autogenous access (AVF), catheters and arteriovenous graft, AVF remains the first choice for HD and was described by Cimino [3]. Prosthetic fistulae become the second option of HD access. Catheters are the latest alternative option [4,5].
VA maintenance requires integration of different professionals to create a team. They should provide their experience in order to give the best options to uremic patients and the best care for their VA [6].
Femoral Vein
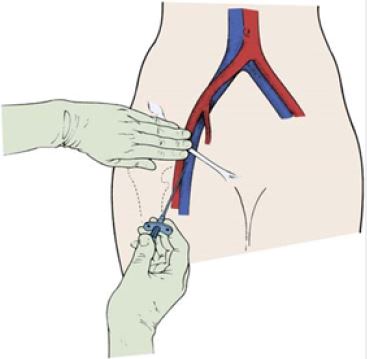
The femoral v catchers are alternative option for hemodialysis. The landmark technique was described for
the first time by Hohn and Lambert in 1966 [7]. The Valsalva maneuver is used to increase femoral vein diameter. It should be taken into consideration that longer catheters increase the resistance of blood flow
[8,9].
Male child aged 4 years old, chronic renal failure on hemodialysis access came to emergency department of
Mansoura new general hospital (international) at September 2018 seeking for dialysis access.
The child’s mother gave a brief history of her child that he did different dialysis accesses before including AVF, temporary and permanent dialysis catheter, jugular, subclavian, femoral and all were exhausted.
The child was stressed, overloaded, in need to urgent dialysis line, and admitted at vascular surgery department for further steps including duplex ultrasound on the venous system of neck and chest and femoral veins.
The duplex result was expected and showed complete occlusion of both subclavians and jugulars, and left femoral vein, the only hope is the right femoral which is partial compressible with few thrombus load.
So the challenge is to put a dialysis access in the right femoral vein, the child transferred to the operative theatre after doing full lab investigations, coagulation profile and other chemical labs.
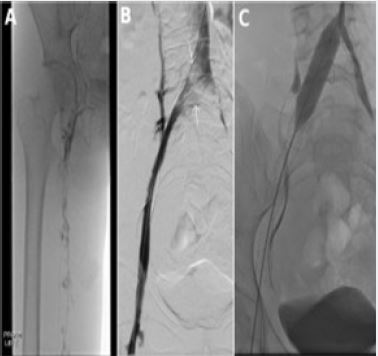
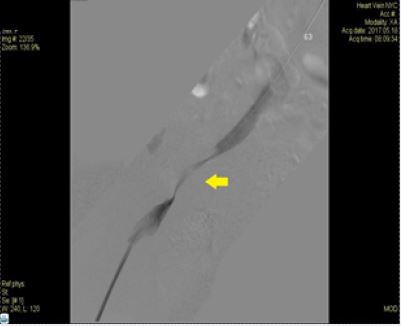
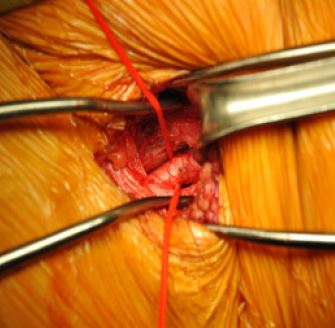
We try to puncture the femoral vein ultrasound guided hardly, we take many trials to do with no satisfactory guide wire pass, finally we did cut down on the right femoral vein and try to pass the guide wire of the dialysis access but there was an obstacle, we did direct venography to diagnose the occlusion/stenosis of femoral vein and iliac, there was a stenosed iliac segment.
We did venoplasty (balloon dilatation) fluoroscopic assisted of the occluded segment by 5 X 6 CM balloon and take flouro image which reveals good perfusion. Finally put the dialysis access over the running wire, and tested its function. Finally we get a line of life for the poor child.
Conclusion
Dialysis access is a line of life for chronic renal failure patient, taking on consideration risks, coast and
benefits is beneficial, with modern endovascular era and revolution, dialysis access became easier, available
and many solutions may appear at any time.
Conflict of Interest
There no financial or personal relationship with other people or organizations that could influence or bias
the content of article
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!