Biography
Interests
Dr. Nasuhi Engin Aydin
Formerly at Department of Pathology, Izmir Katip Celebi University, Izmir, Turkey
*Correspondence to: Dr. Nasuhi Engin Aydin, c/o Pathology Laboratory, Ataturk Hospital, Izmir,Turkey.
Copyright © 2018 Dr. Nasuhi Engin Aydin. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
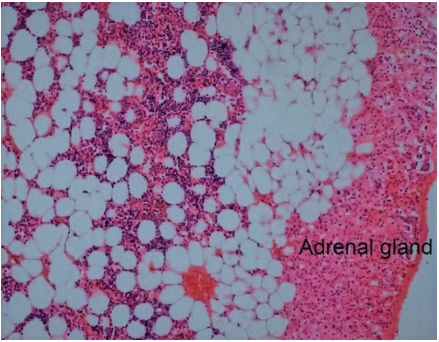
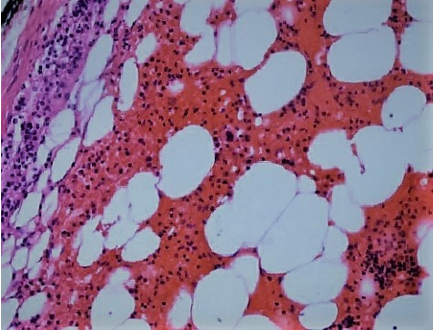
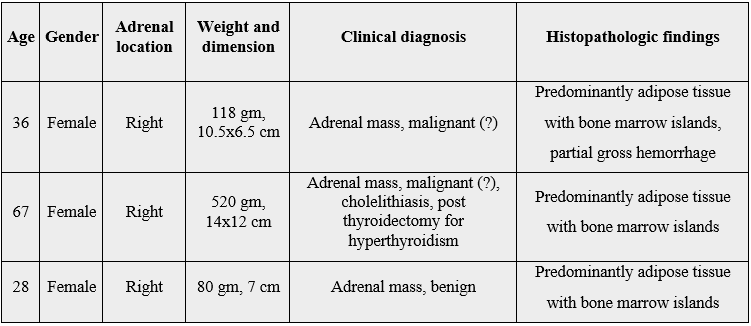
Adrenal myelolipomas are rare benign tumors composed of mature fat and hematopoietic tissue, commonly referred as the second most frequent “incidentaloma” of adrenals. Here three female patients with surgically resected myelolipomas all from the right adrenal are presented. The tissue was biggest in the elderly patient and all were predominantly rich in adipose tissue without any accompanying coincidental neoplasm. All the patients were in good health after a mean follow up period of six years.
Introduction
Myelolipomas (ML) is a rare benign tumor composed of mature fat and hematopoietic tissue with the
most frequent location being the adrenal glands [1,2]. The earliest descriptions date back to the beginning
of twentieth century and were termed as “formations myelolipomatoses” by Oberling in 1929. Thought
to arise from metaplasia of undifferentiated stromal cells, these tumors used to be discovered primarily at
autopsies; however, today they are typically incidental findings in living patients due to the widespread use of
radiologic imaging techniques. Since these masses are asymptomatic and generally discovered unexpectedly
they are also regarded as “incidentilomas” having a high prevalence after adrenal cortical adenomas [1,2].
Case Presentations


Discussion
Mass lesions unexpectedly discovered in adrenal glands are referred as “incidentiloma”. ML is the most
common incidentiloma after adrenal adenoma and comprise approximately 3% of primary adrenal tumors
[1-2]. They are more common in females between fifth and seventh decades of life and in the right adrenal
gland. There is an increase in incidence of reporting this entity in the recent years, about 80% of the cases
reported in the last 20 years and this is assumed to be due to the increased use of imaging modalities
[1-8]. Myelolipomas can rarely appear at other sites of the human body, as well, hence the term extraadrenal
ML [1,2]. Among numerous locations, myelolipomas have been described in the mediastinum,
spleen, kidney, bones, thorax, nasal cavity, ectopic adrenal cortex, as well as at extradural sites or in the
eyes [1,2]. Biochemically, myelolipomas are mostly non-functional. The mean maximum dimension of the
adrenal myelolipoma ranges from 4 to 6 cms [1,2], huge adrenal MLs, i.e. bigger than 7cm, bear a risk
of retroperitoneal hemorrhage [4]. One of the resected tumors among the present series also showed a
partially hemorrhagic appearance (Figures 1 and 2). The patient was operated before developing any clinical
symptoms related to the aggravation of this complication. The three female patients with right adrenal mass
lesions presented here were subject to surgery with successful outcomes without any recurrence after a follow
up period of six and seven years. The two younger patients in this report had laparoscopic surgical approach
with the results reported previously [6]. The older patient who also had gallstones directly underwent open
surgery since the mass was bigger and cholecystectomy was done at the same time. However, she was
hypotensive postoperatively necessitating for a three-day ICU treatment. This was possibly related to the
metabolic status of the patient due to the previous thyroidectomy of nine years ago for hyperthyroidism. The
association of ML with gallstones in this patient seemed coincidental but there is an element of suspicion
regarding a common pathophysiologic basis [5].
There are cases of malignancy coincident with adrenal ML which necessitates meticilous pathologic examination [7,8]. In this regard, it is advisable to have a quick frozen section pathologic assessment intraoperatively to be certain about the nature of a lipomatous mass that seems to be benign. None of the three cases reported here had frozen section despite the fact that in two patients’ presumptive clinical diagnosis included malignancy due to the large dimensions noted.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!