Biography
Interests
Mary Dsane
Department of Dentistry, Volta River Authority Hospital, Ghana
*Correspondence to: Dr. Mary Dsane, Department of Dentistry, Volta River Authority Hospital, Ghana.
Copyright © 2020 Dr. Mary Dsane. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Prevalence of caries in young children is worldwide. Parent perception is a contributor in dental
nonattendance. Reduction in prevalence of periodontal disease help reduce associated systemic
diseases. This research seeks to assess the oral disease burden amongst basic school pupils and the
knowledge, attitudes and beliefs of the people.
The study was a school-based cross-sectional design with 300 study subjects using multi-stage
sampling procedure from four schools. Parents were interviewed on their knowledge, attitude
and behavior towards oral health. Ethical clearance was obtained from Ensign College of Public
Health’s Institutional Review Committee and the Municipal Office of the Ghana Education
Service. Administrative permission was also sought from the heads of the school. Data collected
was be analyzed with Stata.
Prevalence of dental caries was 26.67%, not significant with age, consumption of sweets and drinks,
and frequency of teeth cleaning. DMFT was 1.05 with only a decay component. Periodontal disease
affected 59.33% of the study subjects and was significant with gender and high consumption of
sweets. Prevalence of other oral diseases were low, being higher in rural schools. Parents’ knowledge
and attitude had no significant effect on the outcome of oral diseases.
Oral health of the school pupils is poor and prompt measures need to be implemented to control
the problem.
Integration of healthy oral health behavior into primary health care programs.
Introduction
Oral health is a key indicator of overall health, wellbeing and quality of life. According to the World
Health Organization, oral health is a state of being free from chronic mouth and facial pain, oral and throat
cancer, oral infection and sores, periodontal (gum) disease, tooth decay, tooth loss, and other diseases and
disorders that limit an individual’s capacity in biting, chewing, smiling, speaking, and psychosocial wellbeing.
It contributes to an individual’s wellbeing and quality of life by affecting physical and mental wellbeing
positively, appearance and interpersonal relationships [1]. The public health problems associated with oral
disease are a serious burden on countries around the globe [2] and in spite of the great triumphs in oral
health, burden of oral health diseases remains high in many communities around the world - particularly
among underprivileged groups in high-income and low-income countries [3]. This could be a result of a
myriad of reasons but mainly because of the lack of acceptance of healthy oral habits that are crucial in
preventing the most common oral diseases such as, dental caries and periodontal disease which are considered
as behavioural disease [4]. Countries where oral disease preventive programs have not been implemented
still remain in the shadow of high prevalence of dental caries [5].
Oral disease in children and adults is higher among the poor and disadvantaged population groups. Risk factors for oral diseases include an unhealthy diet, tobacco use, harmful alcohol use and poor oral hygiene, and social determinants [6].
Dental caries and periodontal diseases have historically been considered the most important global oral health burdens. Severe periodontal (gum) disease, which may result in tooth loss, was estimated to be the 11th most prevalent disease globally [7]. It is estimated that 2.4 billion people suffer from caries of permanent teeth and 486 million children suffer from caries of primary teeth globally [8].
A similar situation occurs in Ghana as studies have identified high oral disease prevalence among children. A study in the Tamale Municipality, found a high prevalence of oral disease ranging from 52% to 68% for periodontal disease and 12% to 24% for caries with poor knowledge and attitudes towards oral health [9]. Another in the Ho Municipality showed approximately eighty percent of the children had calculus and gum bleeding. Only 2.4% had visited the dentist in their lifetime whilst 92.9% with dental pain tend to seek selfmedication [10]. Among peri-urban school children in Accra, plaque scores ranged from 78.9% to 97% in the 4-6-year-olds [11].
The general objective of the study therefore, was to investigate the unmet oral health needs of school pupils within the Lower Manya Krobo municipality. To assess the prevalence of oral disease in basic school pupils in the Lower Manya Krobo District and to explore the knowledge attitudes and practices impacting oral health of children in the Lower Manya Krobo Municipality.
Methods
The Lower Manya Kobo Municipal District is one of the 26 administrative districts in the Eastern Region
of Ghana with Odumase-Krobo as its capital. The District covers an area of 304.4 sq km, constituting about
1.7% of the total land area within the Region (18,310km). The major towns in the district include Odumase
township (which incorporates Atua, Agormanya and Nuaso), Akuse and Kpong in the Lower Manya area.
A review of the out-patient department (OPD) cases at Atua Government Hospital of the Lower Manya
Krobo District in the Eastern Region of Ghana from 2016 to 2017 reveals a 3% drop in the patronage of
dental services among children hence the need for investigating the prevalence of oral diseases and knowledge,
attitude and behaviour towards oral health.
The study was carried out using a cross-sectional study design which involved the administration of a questionnaire
and oral examination of school pupils in 4 selected schools in Lower Manya Krobo and the administration
of questionnaire to their caregivers
The sample size of 300 pupils was calculated based on the prevalence of oral disease of 79.6% in a similar study in Ho [10]. The examination was done using an Oral examination tool for school pupils and adolescents modified from the World Health Organization from the Oral Health Survey Basic Methods (5th Edition) The questionnaire sought to obtain information on the knowledge, socio-demographic characteristics, knowledge, attitude and behavior towards oral health among the school pupils and their caregivers. The adult questionnaire included 47 items for the evaluation of the oral health knowledge, attitude and behavior of parents and scored and characterized as excellent, good, average or poor. The prevalence of oral diseases was identified and the KAB of the caregivers.
Prevalence of oral diseases were calculated using the recommended indices DMFTs and CPITN. Pearson
Chi square test was used to test the association/relationship between the prevalence of oral diseases and
socio-demographic characteristics, knowledge, attitude and behaviors among the school pupils and their
caregivers.
Results
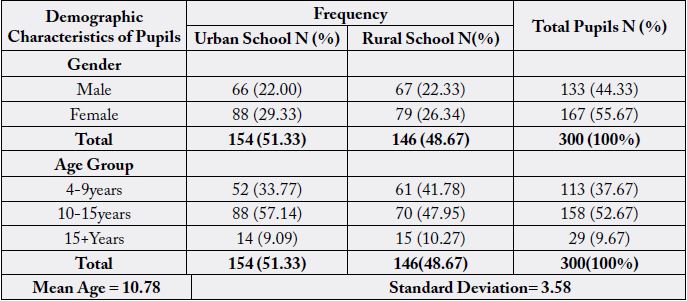
A total number of 300 school pupils between the ages of 4 years and 20 years with the mean age as 10.78
years and standard deviation of ± 3.58 years made up the study population. School pupils belonging to the
age group 10-15 years constituted the greatest percentage (52.67%) of the sample. One hundred and fiftyfour
(51.33%) urban and one hundred and forty-six (48.67%) rural school pupils were examined. Males
constituted 44.33% and females 55.67% of the study population (Table 1).
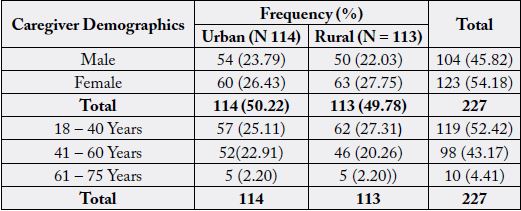
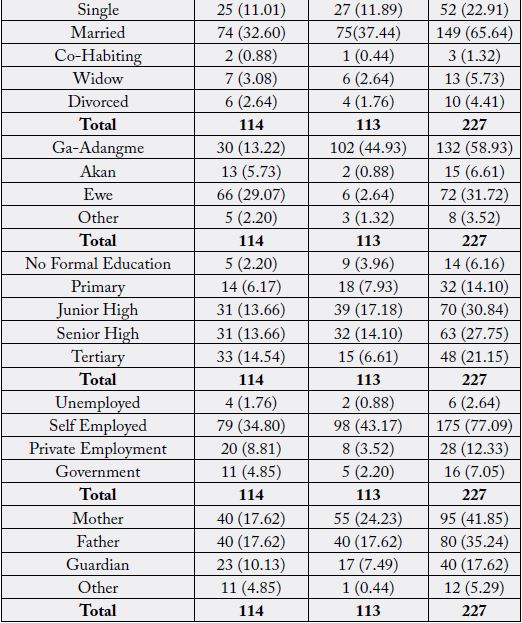
Two hundred and twenty-seven (227) caregivers were effectively sampled out of three hundred (300) giving a response rate of 75.67%. Majority of caregiver respondents were female, 54.19%. The predominant ethnic group was Ga-Adangme which constituted 58.15% of the respondents. Most caregivers had secondary school level education or below, 6.17% had no formal education (Table 2).
From Table 3, the mean DMFT of the study population was 1.05 (±2.68). The minimum and maximum
DMFT recorded were 0 and 22 respectively. Decayed teeth was the only observed component of the DMFT
index. Approximately 73.33% of school pupils were caries free.
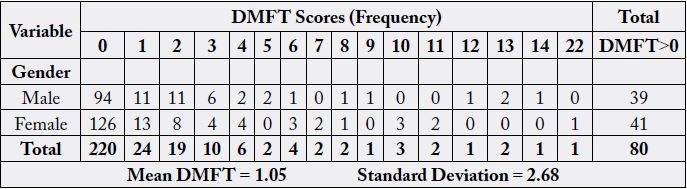
Figure 1 illustrates caries distribution among the age groups. Pupils belonging to 4-9 years age group recorded the most caries prevalence with DMFT score ranging between 0 and 14. The highest DMFT recorded was 22 in the 10-15 year age group. The oldest age group tend to have DMFT score of 0.
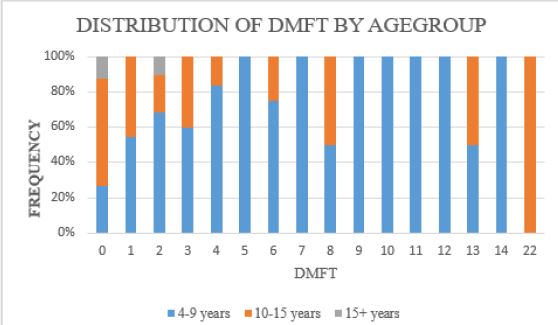
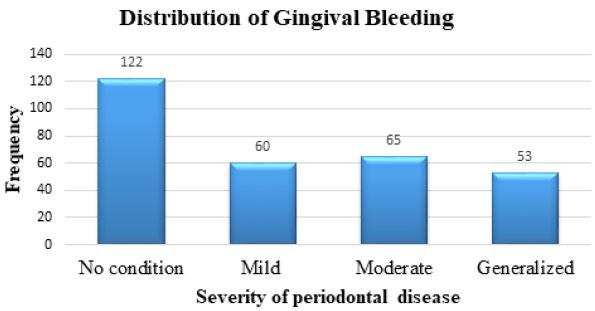
Figure 2 Shows that 122 pupils did not have any obvious gingival bleeding whilst the rest had different degrees of gingiva bleeding. Severe bleeding was identified in fifty-three pupils.
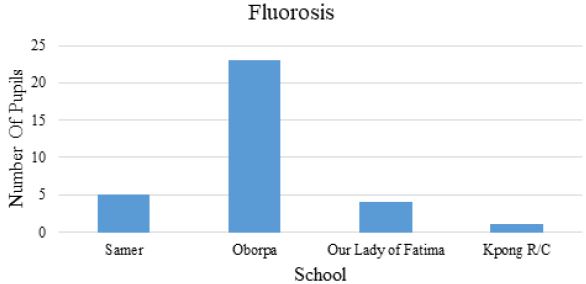
Oborpa school recorded the highest prevalence of fluorosis among the study sample as shown in Figure 3 below:
The most prevalent oral condition was gingival bleeding occurring in 59.3% of pupils. Dental erosion occurred the least, affecting 0.67% of the sample population. Oral mucosal lesions were 2% and 11% respectively. This is shown in Figure 4 below.
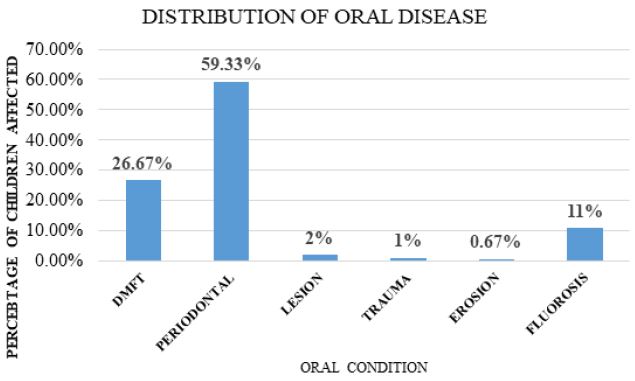
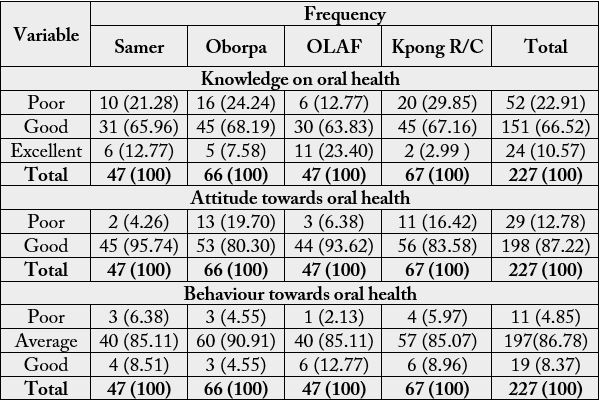
Table 4 showed that oral health behaviour among the guardians was average (Scored between 40-70%). Majority (66.52%) had good knowledge (scored >70%) of oral health. Also, their attitude towards oral health was good. Classification of parents’ knowledge, attitude and behaviour into the groups was adopted and modified from Shabeer Ahamed et al., (2015).
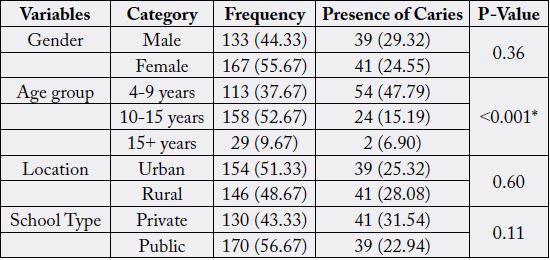
Caries affected 29.32% of males and 24.55% of females. The prevalence of caries had no significant association with gender (p value 0.36). Pupils between 4-9 years were found to have the highest caries prevalence. There was a significant association between caries prevalence and age group (p value < 0.001). There was no significant association between the occurrence of caries and location or school type (p values = 0.60, 0.11 respectively).
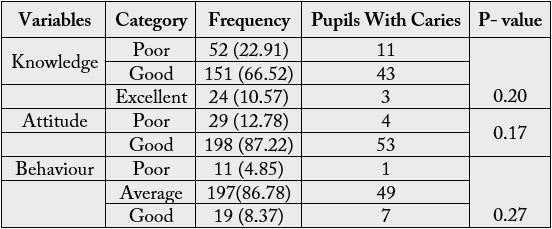
Knowledge, attitude and behavior of caregivers on oral health was not significantly associated with the occurrence of caries among the pupils. Caries occurred mostly among pupils whose caregivers had average knowledge.
Discussion
Human dentition is very important. Its primary function is efficient chewing. Untreated diseases of the
mouth cause dysfunction and eventual tooth loss. The study set out to investigate the unmet oral health need
of school pupils in the Lower Manya Krobo Municipality. The discussion focuses on oral diseases identified
among the pupils as well as the knowledge, attitude and behavior of their caregivers towards oral health.
The main conditions identified included dental caries, bleeding gums, fluorosis, dental trauma and oral
mucosal lesions.
Dental caries is a public health menace in many high-income countries [12] especially among the poor and
marginalized [13]. In developing countries and countries of low socio economic status, dental caries is not as
prevalent [14]. The study showed a DMFT of 1.05 which significantly exceeds the WHO target of DMFT
of below 3 for 12 year olds [15]. This means that pupils in Lower Manya Krobo Municipality have very low
caries incidence, better than what is expected by WHO. This could be attributed to the relatively lower sugar
intake by the school pupils. Majority of these children had never taken in jam. Consistent with this finding,
a study conducted in the Ho Municipality, a district in Ghana with similar characteristics also had low caries
prevalence [10]. The 4-9-year-old group had more frequent caries than the other group. They represented
67% of all pupils with caries experience. This is a matter of concern because they are the children with mixed
dentition and are more likely to have negative effect on both their primary teeth and the permanent teeth.
Gender, location and type of school, whether public or private, did not have any association with the prevalence of caries, with p values of 0.36, 0.60 and 0.11 at a significant level of p<0.05. Age group, however, showed a strong association with p < 0.001. This varies from the Nigerian study which showed a significant association between dental caries and the type of school, p = 0.014 [14]. Pupils with caries showed a strong association with suffering from toothache within the last 12 months, p = 0.042 (p < 0.05). This is similar to results from a survey conducted in Nigeria where 8 to 12 year olds self-reported dental pain which was significantly associated with dental caries with p = 0.04 [14].
It is important to advocate for early intervention to prevent pain and discomfort and to protect permanent teeth from caries experience. The introduction of atraumatic restorative technique (ART) will be of benefit to these children as shown in the 5 year study of children in the South African province of Gauteng [16].
Gingival bleeding occurred in 59% of all pupils. Teeth cleaning and periodontal disease was found to be
statistically significant with age group p - value 0.003. This may be because older pupils are expected to
possess better dexterity than younger pupils thus clean their teeth better. About 60% of children who
brushed their teeth once a day had bleeding gums compared to 59% of children who brushed twice daily.
The frequency of tooth brushing alone, is inadequate in preventing periodontal disease because the skill to
clean well is also very important. It should however be noted that in this study, the caregivers’ involvement
in the cleaning of the pupil’s teeth did not have a significant effect on the prevalence and severity of bleeding
gums, p> 0.504. Meta-analysis done has proven that for improved oral hygiene, there is a need to brush
twice daily for a minimum of two minutes to achieve adequate levels [17].
Periodontal disease is of marked importance due to its association with cardiovascular disease, respiratory disease and diabetes mellitus and also with systemic disease [18,19].
Periodontal disease is expected to increase; hence policy makers need to be proactive in planning towards its prevention. This is because the world population is growing and people are keeping their teeth longer [20].
Prevalence of dental fluorosis was 11% among the school pupils. A large majority of the children with
fluorosis, 23 out of 33, constituting 69.7% were from Oborpa, a rural community with bore hole as their
source of water. Dissolved chemicals such as fluoride can be found in underground water, which when
ingested accumulate in hard tissues such as the teeth and bones and causes fluorosis. Government needs to
ensure the safety of ground water to prevent adverse effects of fluoride [21].
There was a significant association between a pupil having fluorosis and being teased by peers p < 0.03. It is worth noting that fluorosis was not significantly associated with the use of fluoride containing toothpaste, teeth cleaning frequency or satisfaction with appearance of the teeth. It can therefore be deduced that, the fluorosis observed in these pupils is not due to the use of fluoride toothpaste.
Dental trauma was rare, occurring in only 4 pupils. Though the numbers are few, dental trauma is of
significance because of its impact on the sufferer. It affects quality of life of the individual [22]. It forms a
significant portion of trauma occurring globally [23]. Aetiology of dental trauma is varied and wide and
include factors related to the mouth and environment [24].
Oral mucosal lesions were also uncommon. Two pupils had oral abscesses which needed immediate
attention whilst 4 had other mucosal abnormalities. Global prevalence of oral mucosal lesions is much
higher with leukoplakia varying from 0.1% to 10.6% depending on geographical distribution [3]. Some of
the presentation of lesions include dry mouth, discolouration, periodontitis and poor oral hygiene. Among the global goals for oral health 2020, oral mucosal lesions have been targeted for early diagnosis by increasing
the number of health care providers [25].
Changes in diet and lifestyle is associated with the emergence of diseases such as dental erosion, diabetes,
obesity and hypertension [3]. Alcohol consumption, an integral part of many cultures, is also associated with
dental erosion [26]. During the study, only 2 pupils were found to be having erosion of the teeth, though
majority of the pupils drink fizzy drinks several times a week.
Oral disease is the most prevalent non-communicable disease affecting people throughout their lifetime.
It can cause pain and discomfort and sometimes lead to disfigurement and death. The Global Burden of
Disease Study (2016), estimated that oral diseases affect about half of the world’s population, a staggering
3.8 billion people. Periodontitis, characterized by gum bleeding was found to be the 11th most common
disease in the world [27].
It was therefore not surprising that almost all pupils examined had at least one oral disease condition present with only 4.7% of them not needing intervention.
Majority of caregivers had good knowledge of oral health, 66.52%, and a few had excellent knowledge,
10.57%. Attitude towards oral health was mostly good, 78.22%, and behaviour was mostly average. This is
similar to work done in New Delhi, where the awareness of parents and attitudes exhibited regarding their
children's oral health were relatively good. Similarly, there was a need for professional dental intervention,
which was not commensurate with the findings on knowledge, attitude and behaviour, which were good.
This buttresses the fact that knowledge alone is not sufficient if attention is not paid to changing caregivers’
behaviour and attitudes (Kumar et al., 2019). Thus, there is a need to focus on the promotion of healthy
behaviour.
Conclusion
Oral disease is the commonest non-communicable disease in the world. The study identified a high burden of
oral diseases among basic school pupils in Lower Manya Krobo Municipality and the need for professional
intervention appeared to be largely unmet. Though knowledge and attitude towards oral health of pupils
by care givers can be considered as good, behaviour towards oral health is not commensurate and thus the
findings. It is therefore essential to integrate healthy oral health behavior into primary health care programs
such as antenatal and postnatal care to target mothers who form the majority of caregivers and health
educators. Community based Atraumatic Restorative Treatment (ART) services should be introduced at the
community level to improve dental care access.
Limitation of Study
The limitations of this study included caregivers most likely not give factual answers because of social
desirability or conformity. Given that the study was cross-sectional, it may have missed the capture of some
pupils who were exposed to oral health diseases.
The use of only daylight without the aid of radiographs during the oral examination could have resulted in an underestimation of dental caries.
Ethical Consideration
Ethical approval was obtained from the Ensign College of Public Health’s Institutional Review Committee.
Administrative permission was also obtained from the Municipal Education Directorate of the Ghana
Education Service and from Head teachers of the selected schools. Interviewers were trained. Verbal and
written consent was obtained from the school pupils and caregivers selected for the study. Pupils who were
found in need of dental treatment were referred to the Atua Government Hospital. Data was collected
anonymously using identification numbers to ensure accurate pairing/matching.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!