Biography
Interests
Camila Possal de Paula1, Nathale Cruz Batista2, Diego Ribeiro Martins2, Isis Andrea Venturini Pola Poiate3 & Gabriela Alessandra da Cruz Galhardo Camargo4*
1Student of the Dentistry Course of the Institute of Health of Nova Friburgo - ISNF, Brazil
2Student of the Postgraduate Program in Dentistry of the Institute of Health of Nova Friburgo PPGO-ISNF,
Brazil
3Professor of Dentistry, Institute of Health of Nova Friburgo, Brazil
4Professor of Periodontontics, Institute of Health of Nova Friburgo, Brazil
*Correspondence to: Dr. Gabriela Alessandra da Cruz Galhardo Camargo, Professor of Periodontontics, Institute of Health of Nova Friburgo, Brazil.
Copyright © 2019 Dr. Gabriela Alessandra da Cruz Galhardo Camargo, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Gingival recessions can present aesthetic problems, root hypersensitivity, root caries and cervical abrasion and can difficult the plaque control. It can be treated by several periodontal plastic surgery technics, such as subepithelial tissue grafts. Periodontal plastic surgery aims root coverage and can improve keratinized mucosa. Connective tissue grafts in association with coronal advanced flap is reported as the gold standard and does enhance the probability of achieving complete root coverage. However, treatment of gingival recession associated with non-caries cervical lesion presented a challenged to clinician. It may occur due to various mechanisms such as corrosion, stress forces, and friction. Gingival recessions and root abrasion can promote aesthetic problem, dentin hypersensitivity, root caries/demineralization and bacterial plaque accumulation, which are the main indications for the treatment. The objective of this study case report was to evaluate the treatment of gingival recessions associated of subepithelial connective tissue graft as a treatment of Miller’s Class II recession, located in upper right and left canines. A young man was selected for this study, the clinical exam exihibit bilateral recession with no bone loss. The gingival recession was previosly treated by scaling and root planning followed by biomodification with phosphoric acid 37% during 30s for smear layer remotion. The subepithelial grafts were obtaind from the palate, donor area, with a double blade scalpel which promoted benefits in relation to the uniformity of the graft thickness. The subepithelial grafts were associated with the coronal advanced flap technique for both sides. Actually, upper left canine were previously treatement of abrasion lesion with composite resin before the surgical treatment. Clinical results provided successful root covarege after surgical site and surgical/restorative treatment. Both sites were under mantainence during 10 months. It was concluded that Plastic surgical techniques were effective to treat both sites; however gingival recession had not completed tissue coverage, but they have remained stable over a 10-month period.
Introduction
The evolution of dentistry has been occurring over time, acording to the personal needs of patients, aiming
to unite functions, aesthetics, and oral health; Periodontal treatment not focus exclusively on desease and
prevention but also in treatment of reconstructive of tissues loss such as bone and gingiva [1].
Periodontal disease is defined as a pathology involving the periodontal structures of protection and/or support. Clinically, attachment loss can be observed by the presence of periodontal pocket and/or gingival recession. When gingival recession occurs, the apical migration of gingival margin can be detecded and the cementum-enamel junction can be exposed. The gingival recession may be affected one or more tooth and can be classified as localized or generalized [2,3].
Due to the exposure of the radicular caused by the gingival recession, functional alterations of the periodontal tissues and the dental organ can be detected. It is commom observed a greater susceptibility to root caries (decay), dentin hypersensitivity, alveolar bone loss and abfractions [2,4,5].
Among to the diagnoses of gingival recession, the classifications of Miller have been used. Miller suggested four classes: Class I, II, III and IV. The diagnosis considered bone hight and position of dental margin to predict the success of thecnique [6,7]. Cairo classification is another way to diagnosis, which divides into type 1 recession (RT1) that includes Miller’s class I and II, recession type 2 (RT2) added Miller’s classification III, and recession type 3 (RT3) for Miller’s class IV [8,9]. The Cairo classification considers others measures height and thickness of gingival tissues around recessions.
The gingival recessions therapy can be performed by reorientations of dental brushing associated with periodontal maintenance, occlusal adjustments and restorative and surgical procedures. There are several surgical techniques associated with the treatment of recession, including epithelial and subepithelial grafts and lateral repositioned flap that promotes satisfactory results [4,10,11-13].
Based on these, this study aim to evaluate clinical results of gingival recession treatment in superior right canine trated by subepithelial graft technique associated with the coronal advanced flap and left canines treated by subepithelial graft technique associated with the coronal advanced flap and restorative procedure.
Material and Methods
For the present study, it was selected a white young male patient, C.S.C. aged 27 years old. Patient was
selected based on the main complaint, aesthetics, teeth with increased size (figure 3.1). The patient had no
history of smoking or systemic symptoms. After anamnesis and clinical examination the formal consent was
obtained. This study was approved by Ethics Commitee of Human Research of the Intitute of Health of
Nova Friburgo, Rio de Janeiro, Brazil, and it was registered under the number CAEE 87652518.1.0000.5626.
The patients were informed about the protocol of the study and gave their written consent to the described
procedures.

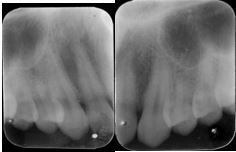
Clinical and radiograpfic exams were performed by experient periodontist. The radiographic exams reveal no alveolar loss around the teehth (figure 3.2) The diagnosis of Miller’s class II recessions were done in anterior upper right (13) and left (23) based on periodontal exams. Probing depth (PD) was 2mm distobuccal, 3mm buccal, and 2mm distobuccal faces, gingival recession (GR) was 4mm at buccal. The clinical attachment levels (CAL) of the respectively sites were 2, 6 and 2mm at upper right canine (13). The left upper canine (23) we observed the presence of abfrations, PS was 2mm mesiobuccal, buccal and distobuccal faces, and GR of 6mm at vestibular face, respectively CAL of 2, 8 and 2mm. No interproximal bone loss and presence of kerathinized tissue apical to root exposed was detected.
Patient was included in a professional oral hygiene procedures were included dental polishing and occlusal adjustment at least 1 week prior to the surgery. All patients were instructed to use a non-traumatic brushing technique (roll technique) with a soft toothbrush. The full-mouth plaque and bleeding scores were under <10% prior the scheduled for surgical procedure.
For the preoperative e postoperative medications, it was used paracetamol 750mg one tablet, one hour before surgery, and maintenance every six hours for three consecutive days and antibacterial control was used chlorhexidine 0.12% daily for each 12h during thirty days.
Surgical procedures were performed under local anesthesia with lidocaine 1: 1000.000 (Composition: 2%vLidocaine Chloridate with Epinephrine 1:1000.000) manufactured by DFL Indústria e Comércio, in Taquara, Rio de Janeiro - Brazil). After, supregingival scaling and root planning (figure 3.5) was performed with 5-6 Gracey currets (Millenium, manufactured by Golgran Indústria e Comércio Instrumentos Odontológicos, in São Caetano do Sul, São Paulo, Brazil). Biomodification was performed with 37% phosphoric acid (Maquira, manufactured by Maquira Indústria de productos odontológicos Ltda, in Maringá, Paraná - Brazil) for 90 seconds (figure 3.6) followed by irrigation with 0.9% saline solution.
The plastic surgery used an intrasulcular incision that was performed with 15C blade (Solidor, manufactured by Suzhou Kyuan Medical Apparatus Co. Ltd, Beiqiao Town, Suzhou City - China) (figure 3.3). Subsequently, the total flap was folded using a molt descaler to exibit alveolar bone (Quinelato, manufactured by: Schobell Industrial Ltda, Rio Claro, São Paulo - Brazil), followed by a partial flap to acess the alveolar mucosa and permit flexibility of tissues (Figure 3.4).




The donor site was palate. The suepithelial graft was prepared with a 15C double blade scalpel (Solidor, manufactured by Suzhou Kyuan Medical Apparatus Co. Ltda, Beiqiao Town, Suzhou, China), a bilaminar incision were performed between the premolars and the first molar regions (figure 3.7 and 3.8) and a kerathinized tissue was removed. After, it was positioned at receptor site and fixed with vicryl 5.0 reabsorbable (Technew, manufactured by Technew Com. E Ind. Ltda., Quintino, Rio de Janeiro - Brazil). The coronal advanced flap was positioned and cover the graft, sutures with nylon 5.0 was performed to maintain gingival margin close to JCE (Technew, manufactured by Technew Com. E Ind. Ltda., Quintino, Rio de Janeiro - Brazil) (figure 3.9).



All this steps was performed at upper right and left canines. The upper left canines had abfraction lesion (figure 3.10). In the place, it was indicated restoration prior to surgery. Before restoration, A2B color with Vita scale was selected (Vitapan, manufactured by Vitapan Indústria Farmacêutica, in Anápolis, Goiás - Brazil).

The restoration was performed under anesthesia 2% lidocaine with epinephrine 1:100.000 (DFL Indústria e Comércio, Taquara, Rio de Janeiro - Brazil) followed by preparation with diamond drill 2200FF (KG Sorensen, Medical Burs Indústria e Comércio de Produtos abrasivos Ltda., In Cotia, São Paulo, Brazil) (figure 3.11). Subsequently, the biomodification was performed using phosphoric acid 37% (Maquira, manufactured by Maquira Indústria de productos odontológicos Ltda, in Maringá, Paraná - Brazil) for 30s at enamel and 15s at dentin, according to the manufacturer's information. The surfaces were washed and dried (Figure 3.12). The two-step adhesive was selected (Adper Single Bond 2 Adhesive, manufactured by 3M do Brasil Ltda, Sumaré, São Paulo - Brazil). First step, primer were applicated for 30s followed by second step, adhesive were applicated for 60s, both were photopolymerized for 20 seconds, according to the manufacturer's information (figure 3.13). The A2B color microparticulate resin filled in layers (Filtek Z350 XT, 3M do Brasil Ltda., Sumaré, São Paulo - Brazil), by incremental technique and photopolymerized for 20 seconds, according to the manufacturer's instructions.



The final result was carried out in the same session with the drills 3195FF, 2135F and 3168FF (KG Sorensen, Medical Burs and Abrasive Products Trade Ltda., Cotia, São Paulo, Brazil) and polishing tips for resin (10,204,015), medium (10,204,016) and thin (10,204,011) (Microdont, manufactured by 3R Ind. E Com. Ltda., in São Paulo, São Paulo - Brazil) respectively with the paste (TDV, manufactured by TDV Dental Ltda., in Pomerode, Santa Catarina - Brazil) (figure 3.14).

After seven days, nylon suture 5.0 was removed (Technew, manufactured by Technew Com. E Ind. Ltda., Quintino, Rio de Janeiro - Brazil). The Vicryl wire remained in place until its reabsorption. The follow-up periods were seven days (Figures 3.15 and 3.16), three months (Figures 3.17 and 3.18) and ten months (Figures 3.19 and 3.20) of postoperative follow up.






Results
The results are arranged in figures. Initial aspects (figure 3.1) and immediate postoperative period (figure
3.9 and 3.14) and postoperative follow-up periods (Figure 3.19 and 3.20), it was possible to note aesthetic
improvement, reduction of gingival recession. The upper right canine presented probing depth (PD) with
2mm in the mesiobuccal, buccal and distobuccal, gingival recession (GR) 1mm at buccal, clinical attachment
level (CAL) was 3mm for all buccal faces after 3 and 10 months. The gingival recession reduced 3mm at
buccal face. The upper left canine presented probing depth (PD) with 2mm in the mesiobuccal, buccal
and distobuccal, gingival recession (GR) 3mm at buccal, clinical attachment level (CAL) was 2mm for
mesiobuccal and distalbuccal, 5mm to buccal faces after 3 and 10 months. The gingival recession reduced
3mm at buccal face.
Discussion
This study observed that the subepithelial connective graft was efficient for the root coverage of the upper
canines diagnosed with Miller's class II recession. However, results did not reveal complete coverage after
surgical procedure.
According to Aroca et al. (2009) [14] dental localization is an important parameter that can affect the surgical results; anterior teeth tend to present better results than posterior teeth. In this study, anterior teeth were selected for the treatment of root coverage and good results were obtained.
Zucchelli et al. (2018) [13] suggested that the amount of keratinized tissue apical and laterally, as well as gingival thickness may have an impact on complete root coverage. However, these measures were not performed in this study. The presence of probing depth, gingival recession and clinical level of insertion were observed. The success of the technique was evaluated by reducing the gingival recession that was observed both sites. The clinical results of the follow up of this study allowed observing that the results obtained with 3 months were maintained until the period of 10 months and that the removal of the causal factor and good oral hygiene were primordial to maintain the results obtained and improved the prognosis of the case.
Regarding to the technique of graft removal, the authors reported that there are differences in the constitution of connective tissue, variations from patient to patient may occur both in thickness and percentage of lamina propria and submucosa, as well as differences in thickness from the anterior to posterior region of the palate. Harris (2003) [15] reported the thickness variation obtained by histological analysis can vary from 65.2% of lamina propria and 34.8% of submucosa in grafts obtained with double lamina scalpel. Eustachio (2018) [6] reported that connective tissue grafts are rich in collagen fibrils mainly type I and II, suggesting a lower level of contraction, but a greater difficulty in revascularization and the possibility of scar remaining in the recipient layer. The author reports that this probably occurs due to epithelial remnants left during the desepithelialization. In this work, it was not possible to perform histological analysis of the connective tissue, since the subepithelial tissue graft was removed with a double-blade scalpel and immediately sutured at the receptor site.
In relation to tissue coverage on at upper canines Zucchelli et al. (2006) [16], considered the decrease of the percentage of tissue coverage occurs due to the alterations in the cervical region. According to the authors, the cement-enamel junction disappears due to the destruction of cervical lesion and the line that divides the end of the enamel and the coronary dentine become exposed. This line represents an angle of the noncarious lesion and is often confused with the cementum- enamel junction. After the restoration has been made, the cervical line, cemento-enamel junction may disappears, as they become covered by the restoration and there is a tendency to cover only the root portion of the root, so that the coronary portion tends to be discovered, which causes a decrease of the tissue coverage percentage. The authors also concluded that making comparisons of percentage of root coverage of elements with non-carious cervical lesion with elements that have the complete or restored cervical portion is erroneous. In disagreement with this statement, Santamaria (2007) [17] reported that the presence of resin-modified glass ionomer restoration applied in non-carious cervical lesion does not interfere with the coating percentage.
In relation to the biomodificación of the root surface, in vitro studies using conditioning agents for the root surface show a great variability of the results due to the variety of conditioning materials used such as citric acid, phosphoric acid and tetracycline hydrochloride and that these agents have low pHs that may interfere with pulp vitality and gingival tissue [18]. Ethylene diamine tetra-acetic acid (EDTA) was highlighted in studies comparing this agent to citric and phosphoric acids, as it showed no induction of any pulpal alteration [19,20]. In addition, these agents were more efficient in the removal of smear layer and exposure of collagen fibers of dentin and cement. However, despite appearing to be an ideal agent after in vitro studies, EDTA began to show adverse effects, since this agent is a strong calcium ion chelator, which hindered or even inhibited the first step in the attempt of periodontal regeneration / repair, which is the formation of the clot. Studies with tetracycline hydrochloride are widely used and present good results [21]. However, this study selected 37% phosphoric acid to induce root biomodification due to its ease of availability, but also to obtain results, since few studies report its use for this purpose [22].
Based on the results obtained in this study, it was concluded that the subepithelial connective tissue graft was efficient for the treatment of gingival recessions for a period of 10 months, however, gingival recession had not completed tissue coverage, but they have remained stable over a 10-month period.
Conclusion
Plastic surgical techniques were effective to treat both sites; however gingival recession had not completed
tissue coverage, but they have remained stable over a 10-month period.
Acknowledgments
We thank the Postgraduate Program in Dentistry of Nova Friburgo Health Institute PPGO-ISNF and the
Coordination of Improvement of Personnel of Higher Education CAPES.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!