Biography
Interests
Anoop Kumar1, Nithya Jagannathan2* & Yekkoluku Nagaranjitha2
1Department of Oral and Maxillofacial Pathology, PSM College of Dental sciences and Research, Trichur, Kerela,
India
2Department of Oral Pathology, Saveetha University, India
*Correspondence to: Dr. Nithya Jagannathan, Department of Oral Pathology, Saveetha Dental College, Chennai, India.
Copyright © 2018 Dr. Nithya Jagannathan, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
The aim of the study was to establish a relationship of dental caries with the GTF and streptococcus
mutans count to determine the caries active individuals.
The study comprised of 40 children, of which 20 were clinically diagnosed as having early carious
lesions and the rest were clinically free of caries. About 2ml of unstimulated saliva was collected
from the study group and the control group. The salivary sample was uniformly mixed and about
1.5ml of saliva was streaked on the Blood agar and chocolate agar supplemented with bacitracin,
using a 4mm inner diameter inoculation loop. The MSR agar plates were incubated anerobically for
48 hours at 37 degree celcius. Following the incubation, counts were made from the colonies which
had morphologic characteristic of Streptococcus mutans on the MSB agar. Glucosyltransferase activity was measured using DNA assay.
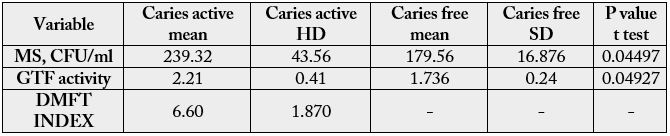
The mean DMFT of the study population was 6.60 with a standard deviation of 1.870. The mean
number of decayed, missing and filled teeth were 4.0 ±1.8, 0.5±0.23 and 2.1 ±0.6 respectively. The
Mean streptococcus mutans count in caries free subjects was 179.56x 103 ± 16.876 x103 and in
subjects with carious lesions the mean mutans count was 239.32x 103 ± 43.56 x103.
Glucosyltransferase serves as a potential marker for predicting the caries active individuals. A
correlation between Glucosyltransferase activity and DMFT index also correlates with our results
proving that GTF could act as an ideal marker for dental caries.
Abbreviations (if used)
DMFT - decay, missing and filled tooth
GTF - Glucostltrasferase
WHO - World Health Organization
Introduction
Dental caries continues to be a major public health problem in global proportions despite overly attempts
undertaken in the elimination of the disease [1]. It is indeed true that the prevalence of dental caries has
declined in developed countries [2]. However, the prevalence in children ranges from 33.5% to 90% in Indian
population and continues to be a public health challenge [2]. Streptococcus mutans is a predominantly
common oral bacterium present in virtually all individuals and it is well known that a causative association
exists between streptococcus mutans and dental caries [3]. This is facilitated by Glucosyltransferase (GTF)
an enzyme produced by streptococcus mutans which plays a crucial role and is arguably the most significant
virulence factor in dental caries [4]. GTF utilize an activated donor sugar substrate containing a substituted
phosphate group [5]. They catalyze the formation of glycosidic bonds from sucrose and thus play a role in
the etiology of dental caries by mediating the adherence of Streptococcus mutans to the tooth [6].
GTF is present in whole saliva and it also enables the formation of dental caries. Salivary GTF is produced by S. sanguis, S. sorbinus and S. mutans [7]. Diagnosis of caries rely commonly on visible, radiographic and tactile methods and the lesions diagnosed in this way are quite advanced and several stages of bacterial succession may have taken place between caries initiation and its subsequent diagnosis [7]. An ideal caries activity test is one that could determine caries activity prior to the onset of lesions. The study was performed to establish a relationship of dental caries with the GTF and mutans count to determine the caries active individuals.
Materials and Methods
The study comprised of 40 children, of which 20 were clinically diagnosed as having early carious lesions
and the rest were clinically free of caries at the time of their dental identification. All the subjects were from
the same school, indicating that they were from the same area with same socioeconomic status. The subjects
were examined under natural light in an outdoor setting following an oral rinse, with the aid of a plane
mouth mirror and CPI Probe, according to the criteria recommended by the World Health Organization
(WHO). All the erupted teeth were evaluated using the DMFT index for the permanent tooth. White,
chalky and discoloured spots with absence of visual cavity and stained pit and fissures that did not have
undermined enamel was not recorded as caries and were excluded from the study.
About 2ml of unstimulated saliva was collected from the study group and the control group. Donors were
asked to refrain from eating or drinking for at least 60 minutes prior to each collection. Smoking, chewing
gum and intake of beverages were also prohibited during this hour. The subjects were asked to rinse the
mouth with deionized distilled water and were supplied with a sterile container. Briefly, after a rinse of the
mouth with water, saliva was allowed to accumulate in the floor of the mouth for approximately 2 minutes
and the subjects were asked to expectorate the unstimulated saliva into the sterile container. Following
collection, the samples were aliquoted and the samples were then centrifuged at 2500rpm for 5 minutes.
The centrifugation resulted in saliva samples free of large particulate debris and reduced viscosity, thereby
allowing a more accurate and reproducible analysis. The supernatant was subsequently stored at -30°C until
analysis was performed [8].
The salivary sample was uniformly mixed and about 1.5ml of saliva was streaked on the Blood agar and
chocolate agar supplemented with bacitracin, using a 4mm inner diameter inoculation loop. The MSR agar
plates were incubated anerobically for 48 hours at 37degree celcius. Following the incubation, counts were
made from the colonies which had morphologic characteristic of Streptococcus mutans on the MSB agar.
The identification of streptococcus mutans was confirmed by mannitol fermentation. The number of mutans
colonies were determined and multiplied by 10 as the saliva was diluted.
The broth supernatant was collected from the culture and inoculated in thioglycollate broth at 37 degree celcius and the supernatant was obtained. The supernatant was further centrifuged to remove the sediments and for further analysis.
The amount of glucosyltransferase was determined by Dintrosalicylic acid assay.. One unit of glucosyltransferase
is defined as the amount of enzyme that catalyzes the production of 1 micro mol of fructose per min. at 30 degree C in 20mM sodium acetate buffer, pH 5.4, with 100g of sucrose per liter, 0.05g of CaCl2 per
liter, and 1g of NaN3 per liter. It was ascertained that the reducing sugar measured by DNS assay was due to
glucosyltransferase and not to levansucrase, inveratase, or sucrose phosphorylase activity.
Results
The mean DMFT of the study population was 6.60 with a standard deviation of 1.870. The mean number of
decayed, missing and filled teeth were 4.0 ±1.8, 0.5±0.23 and 2.1 ±0.6 respectively. The Mean streptococcus
mutans count in caries free subjects was 179.56x 103 ± 16.876 x103 and in subjects with carious lesions the
mean mutans count was 239.32x 103 ± 43.56 x103.
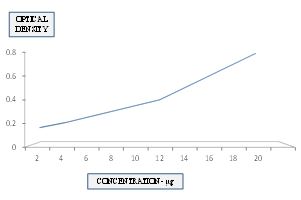
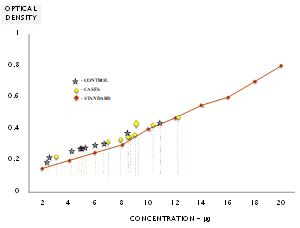
A graph was plotted with the optical density along y axis and the standard concentration along x axis for spectrophotometric determination of the optical density of standard solution. The concentration of the reducing sugar was thereby obtained by marking the optical density of the reducing sugar obtained by spectrophotometer on the graph of standard solutions and thereby correlating it with the concentrations on the x axis.
Statistical analysis was done using regression analysis and Spearsman Correlation coefficient due to non
linearity of the distribution. The p value of streptococcus mutans in caries active and caries free was 0.44
and the GTF levels in caries active and caries free individuals was 0.49 which suggests that there 95%
significance. The Regression analysis for DMFT versus S.mutans was 0.75 and DMFT versus GTF was 0.9.
Discussions
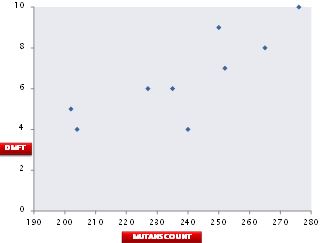
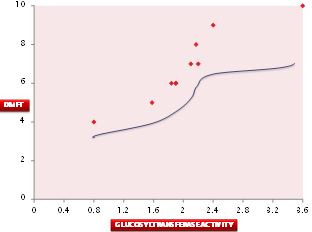
Our study established a strong correlation between the Glucosyltransferase activity DMFT and a moderate
correlation between Streptococcus mutans and DMFT index. This could be attributed to the individual
indices of the DMFT. Our data revealed a patient with 7 decayed teeth and 3 filled teeth contributing to
a DMFT index of 10. The Glucosyltransferase activity was significantly increased to 3.8 with S. mutans count of 276. However another case with DMFT score of 9 had 3 decayed teeth, one missing tooth and 5
filled teeth. The Glucosyltransferase activity was 1.9 with S. mutans count of 245. This suggests the variation
in Glucosyltransferase levels with the Decayed teeth present in DMFT index. This suggests that a direct
relationship exists between DMFT and streptococcus mutans and DMFT index (Graph 3 and Graph 4).
Our data represent an essential first step in developing a simple and reliable caries activity and predictive test. The strong correlation between lesions and Gtf is certainly encouraging. Our study revealed a strong correlation between the level of Gtf, with the number of clinical lesions of our pediatric subjects.
The ability to measure the level of a proven virulence factor and correlate it with clinical caries activity represents a step forward toward using the assay to aid in diagnosis of caries before overt lesions are present.
Our data confirmed previously reported correlations between salivary MS populations and dmfs. The correlation between salivary Gtf and dmfs appears to be stronger than that between MS and dmfs. Gtf as a potential marker for caries activity has considerable advantages over cultural methods and other approaches such as PCR. Gtf is a proven virulence property of S. mutans [9,10]. Therefore, the test proposed here includes an agent directly involved in the pathogenesis of the disease. The test as envisaged could be used chair side and provide results within minutes. It is difficult to imagine primer and PCR mutans counts being used chair side, however carried out, as they require days to develop and need some laboratory equipment. In addition, as Bowden [1997] pointed out, cultural methods do not differentiate among clonal types which may or may not be associated with virulence. This observation may also in part account for the relatively poor performance of MS counts as predictors of caries development. It may also explain why a correlation between MS counts and Gtf was not observed in this study.
Conclusions
An ideal test for caries activity is one that could determine caries activity prior to the onset of lesions. The
best predictor of future caries experience thus far involves assessing the presence of carious lesions already
present on tooth surfaces which from a clinical perspective is rather late ECC constitutes a major public
health problem and affects those who are least able to bear either the financial or health burden. Children
in underserved areas visit a physician more readily than a dentist [11]. If a simple test is developed, such
as described here, it could be used by the physician to screen the children for caries risk during ‘well child’
visits and then make appropriate referrals of those identified as high risk to a dentist for the institution
of preventive procedure, perhaps reducing the incidence of dental caries, obviating the need for extensive
restorative care.
Acknowledgements
The authors thank Dr. Niranzena Pannerselvam, Department of Radiology, University of Florida for her
support in publishing this article.
Conflicts of Interests
The authors report no conflict of interest
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!