Biography
Interests
Amir Khalid
Qatar Armed Forces, Doha, Qatar
*Correspondence to: Dr. Amir Khalid, Qatar Armed Forces, Doha, Qatar.
Copyright © 2018 Dr. Amir Khalid. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
The achievement of full mouth rehabilitation is the main goal of patient and dentist, and the use of implant
for such a purpose is an attractive alternative procedures [1-4]. The main target of Implantology is to achieve
patient’s comfort and esthetic throughout their healing phases till the final restoration [5,6], and maintaining
the facial vertical dimension [7]. Incorporation of fixed prosthesis retained by implants and a removable
prosthesis using a very fine delicate precision attachment (MK1) allow the patient to have a more pleasant
and stable treatment and the patient will experience a less trauma. The vertical dimension of occlusion may
be maintained, in addition to continued support of the facial structure.
The Case
A 66-year-old male attending the Gharafa Medical Complex in Doha, Qatar seeking an advice and treatment
for his lower jaw prosthodontic problem. Clinical examination revealed a very carious and fractured  and poorly covered by a cantilevered bridge extending from 5 ← 1 area. The 3 was endodontically treated
and crowned, and the lower left area is completely edentulous.
and poorly covered by a cantilevered bridge extending from 5 ← 1 area. The 3 was endodontically treated
and crowned, and the lower left area is completely edentulous.
Radiographical examination revealed, presence of a periapical changes underneath 321 with a wide area of
boney ridge resorbtion as well as the presence of the first step of two stage implant IMZ system at the area
of  and
and  .
.
These two implants were laid and left without completion since 10 years, so they are completely barried by
bone. The treatment plan was simply made to remove the cast bridge covering with their teeth and to
restore  then to do implant therapy for the lower right area by using ITI (straumann) transgingival system.
SLA (sand blasted, large grite, acid etched) type was chosen to get shorten the time to load and to increase
the success rate of the work [7,8,9]. Complete the implant for lower left area as a full mouth rehabilitation
attempt.
then to do implant therapy for the lower right area by using ITI (straumann) transgingival system.
SLA (sand blasted, large grite, acid etched) type was chosen to get shorten the time to load and to increase
the success rate of the work [7,8,9]. Complete the implant for lower left area as a full mouth rehabilitation
attempt.
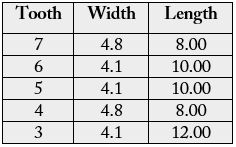
It is advised to use an implant for each missing posterior tooth where the bone is favorite even in a staggered (offset, tripodisation) configuration to decrease bio-mechanical complications [7]. However, Halden et al [8] found by the use of three implants of 4.1mm in diameter and 10mm length kept the stress distribution within the normal limits.
In this case it was decided to use one implant for each missing posterior tooth of the lower right region as Table (1).


ITI solid screw SLA implants were laid in the area of  and a surgical extraction of was made
and removing all the infected, granulated tissue and remanents of remaining periodontal ligament and
doing guided tissue regeneration procedure with the aid of deminerlized freeze dried bone using (bone-oss)
and an absorbale regenerative barrier to prevent epithelial migration into the ridge site using (bone-guide)
absorbable membrane.
and a surgical extraction of was made
and removing all the infected, granulated tissue and remanents of remaining periodontal ligament and
doing guided tissue regeneration procedure with the aid of deminerlized freeze dried bone using (bone-oss)
and an absorbale regenerative barrier to prevent epithelial migration into the ridge site using (bone-guide)
absorbable membrane.
Lastly the implant in  area was laid after checking the success of the tissue regeneration in the area of
area was laid after checking the success of the tissue regeneration in the area of
 after waiting a period of six months. The area in
after waiting a period of six months. The area in  was not suitable for implantation. However, it is
completely healed and calcified.
was not suitable for implantation. However, it is
completely healed and calcified.
Unfortunately, all our trials to find the abutments of the transmucosal interpore IMZ (4.0mm) implant on
area abutments of the  due to its internationally out of stock, this put us in face of two options, either to
remove the implant and implant a new ITI implants or to leave them and replace it by removable prosthesis.
The patient prefers the second option due to its faster result.
due to its internationally out of stock, this put us in face of two options, either to
remove the implant and implant a new ITI implants or to leave them and replace it by removable prosthesis.
The patient prefers the second option due to its faster result.
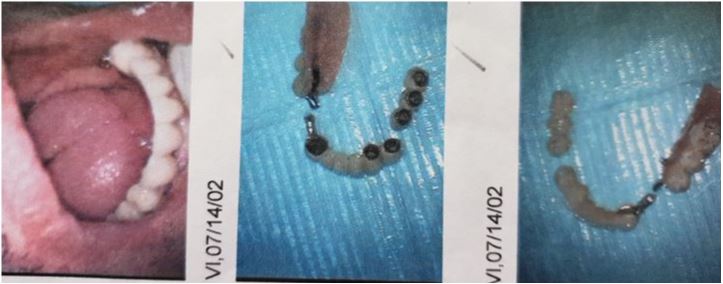
Therefore, the has been restored and crowned by full veneer porcelain crown to which part of a newly
designed precession attachment called MKI was attached, while the female part was attached to a cobalt -
chromium partial denture.
This attachment is ready fabricated to achieve the balance and requirements of function, hygiene and esthetics in the oral environment. It is rigidly connected to natural abutments or implants using the premilled female and milled lingual arm, transferring chewing forces to the central axis of the abutment during insertion and withdrawal of the prosthesis.
The prosthesis has been placed, adjusted and monitored for four months without any complaints.
Patient did not have any medical complication because she had a new medical checkup 10 days ago. So, the likelihood of allergy due to medical illness cannot be the reason for this problem.
During the treatment time, the patient was wearing a temporary full denture fabricated with cold cure acrylic lined by soft tissue liner to avoid premature pressure being placed on the newly implanted area. The patient was instructed to refrain from its use for seven days after each implant surgery.
Discussion and Conclusion
The importance of dental treatment is very much essential now. This technique is highly recommended and
is been used for 10 years now without any clinical problem.
However, most of the patients cannot continue the implant treatment therapy due to tiredness or could not afford the treatment financially.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!