Biography
Interests
Emmanuel Chioma Blessing1* & Rita Ramos, C.2
1Nursing Science Department, Imo State University Owerri, Nigeria
2University of the Philippines Open University, Los Banos Philippines
*Correspondence to: Dr. Emmanuel Chioma Blessing, Nursing Science Department, Imo State University Owerri, Nigeria.
Copyright © 2018 Dr. Emmanuel Chioma Blessing, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Every newborn needs essential care which must be initiated as soon as the baby is born and continued for at least the first month of life. In the absence or less of this care, new born morbidity and mortality may occur.
To determine the level of maternal competence of essential new born care, identify factor influencing
the maternal competence level of postnatal mothers, and examine the relationship between maternal
competence and selected socio-demographic variables.
Exploratory design was used in this study. A purposive sample size of 76 postnatal mothers
participated based on the inclusion criteria. Parenting Sense of Competence (PSOC) scale was
used for data collection for this study. Data were analyzed using descriptive statistics and chi-square
test for the relationship between maternal competence and socio-demographic variables at p<0.05
level of significance.
Maternal competence was high in efficacy (4.36) but low in satisfaction (3.73). Factors identified
as influencing maternal competence are traditional beliefs (35.5%), social status/income (65.8%),
Place of antenatal/delivery (64.5%), Mothers’ health status (78.9%), and stress (57.9%).
Essential newborn care should be part of antenatal education programme and health promotion
campaign that is based on these factors influencing maternal competence should be implemented.
Introduction
Global deaths of newborn babies remain alarmingly high, particularly among the world’s poorest countries
[1]. Every year, 2.6million newborns around the world do not survive their first month of life. One million
of newborn child die the day they were born [1]. Owoseye (2017) reported that Nigeria was third (9%)
among the five countries who accounted for half of all newborn deaths worldwide in 2016 [2]. According
to National Bureau of Statistics of Nigeria [3] & UNICEF (2018) [1], Nigeria experienced 37 deaths per
1,000 births in 2017 and more than 80 percent of these newborn deaths were associated with prematurity,
complications during birth or infections such as pneumonia and sepsis. These deaths can be prevented with
access to well-trained midwives, along with proven solutions like clean water, disinfectants, breastfeeding
within the first hour, skin-to-skin contact and good nutrition. Bala, Devi & Gomathi (2013) submitted that
every year more than four million babies die during their first week of life due to inadequate care by mothers
or caregivers [4].
Every newborn needs essential care which must be initiated as soon as he/she is born and continued for at least the first month of life. This care can be provided by the health care professionals, trained community health workers, support persons and /or the mothers in the hospitals or at homes. In the absence or less of this care, newborn morbidity or mortality may occur. Essential newborn care includes basic preventive care, early detection of danger signs and treatment of problems such as sepsis and birth asphyxia [5]. Basic care for all newborn should include promoting and supporting early and exclusive breastfeeding, keeping the baby warm (prevention of hypothermia), increasing hand washing, baby bathing, providing hygienic cord and skin care and immunization [6,7]. Newborn care and care seeking behavior at the right place and on time are always the responsibilities of the caregivers at home.
According to Emmanuel et al (2017), adequate care of the newborn baby depends on the mothers awareness, attitude and skills, thus maternal competence is vital [8]. Women with a strong sense of competence and satisfaction in the maternal role had a secure attachment style, sensitive and response nurturing behavior which facilitates the infant’s growth and development [9]. Maternal competence was low in the aspect of satisfaction among Nigerian mothers [8]. Shrooti et al (2016) emphasized that women’s achievement of competence in the maternal role involves multiple factors such as age, socio-economic status, self-concept, childrearing attitudes, previous experience with child, maternal and infant health status, family functioning, stress and support system which are in turn influenced by a woman’s social and cultural background [10].
Identifying these factors in this area of study is necessary in order to design and implement sustainable interventions to reduce infant /child mortality by two-third from 2010 to 2030 in Nigeria and globally [11]. Therefore, we aim at determining the factors influencing maternal competence of postnatal mothers and examine the relationship between maternal competence and the socio-demographic variables among a sample of Nigerian mothers.
Materials and Methods
The specific objectives of this research include:
• To determine the level of maternal competence of postnatal mothers according to efficacy and satisfaction.
• To identify the factors influencing maternal competence of postnatal mothers.
• There is a significant relationship between the maternal competence of postnatal mothers and the maternal
age, parity, educational level, occupation, family support persons, area of living and marital status.
This study was based on Ramona Mercer becoming a mother theory which was formerly known as the
theory of maternal role attainment. It focuses on the mother’s role identification and role competence.
The mother experiences satisfaction in her role as she gains confidence and competence in responding and
providing care to her infant [12].
An exploratory design was used in this study with one focus group (postnatal mothers). The data was
collected as part of a quasi-experimental study on the effectiveness of newborn care programme on perceived
maternal competence and satisfaction [8].
This study was conducted in the postnatal ward of Imo State Specialist Hospital Owerri, Nigeria. The
hospital records an average of 40 - 80 deliveries every month. Women within Owerri and nearby rural areas
utilize the services of this hospital.
Approval by the research/ethical committee of the hospital was obtained. Written and verbal information
were given to the mothers about the study for their voluntary participation. To ensure privacy and anonymity,
numbers and alphabets were used on the questionnaires instead of respondents’ names. All the participants
gave their consent and data were confidentially treated. Permission was also given by the developer of the
instrument used.
The population was mothers who delivered in this hospital within the one month of this study. Sampling
was purposive. The inclusion criteria were postnatal mothers with term safe vaginal delivery (SVD), low risk
pregnancy, who are willing to participate, at least 18years and competent to consent. 76 mothers who met
the inclusion criteria formed the total sample size.
The instruments used to collect data were:us.
A. An 8- item questionnaire containing socio-demographic data and open-ended question on factors influencing maternal competence. The socio-demographic variables considered were age, occupation, educational level, parity, area of living, family support persons and marital status. For the open-ended questions, mothers were given the opportunity to write other factor influencing their newborn care maternal competence level.
B. The 16- item Parenting Sense of Competence Scale (PSOC) developed by Gibaud-Wallston and Wandersman (1978) which measures maternal competence in two dimensions: Efficacy subscale (PSOC-E) OF 7 items and Satisfaction subscale (PSOC-S) of 9 items [13]. The scale ranges from 1 (strongly disagree) to 6 (strongly agree). The result of this study was interpreted based on high and low levels using the mean score. Mean score of 3.99 and below is low level while 4 and above is high level of competence. Internal consistency of PSOC is 0.82. Gilmore and Cuskelly (2008) recorded internal consistency of 0.72 (mothers) and 0.76 (fathers) [14]. 76 questionnaires were distributed to these mothers between 2-4 days after delivery and collected immediately after filling them. The researcher visited the hospital every other day to meet mothers before discharge.
Analysis of the data was done using Statistical Package for Social Sciences (SPSS) version 20.0. Descriptive
statistics (frequency, percentage, mean, and standard deviations) and chi-square test for the relationship
between maternal competence and socio-demographic variables.
Findings

Table 1 above presents the total score of M=30.5 and SD=10.905 with total mean score of 4.36. This shows high level of efficacy in the maternal competence of postnatal maternal mothers.
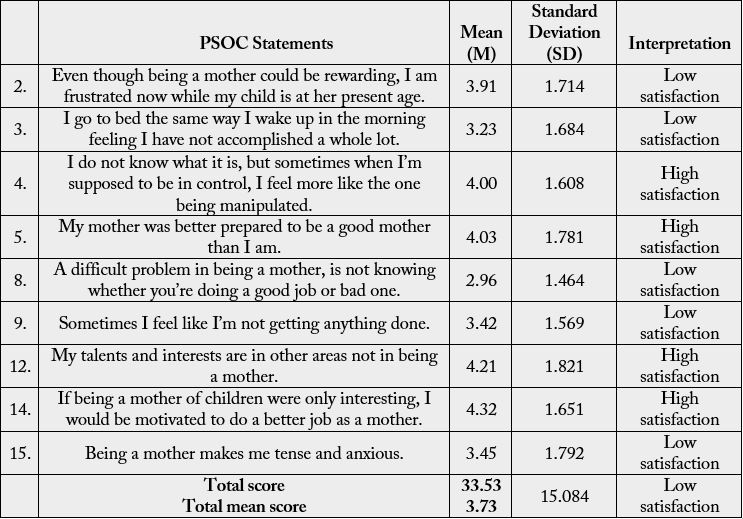
Table 2 above presents the total score of M=33.53 and SD=15.084 with total mean score of 3.73. This shows low level of satisfaction among postnatal maternal mothers.
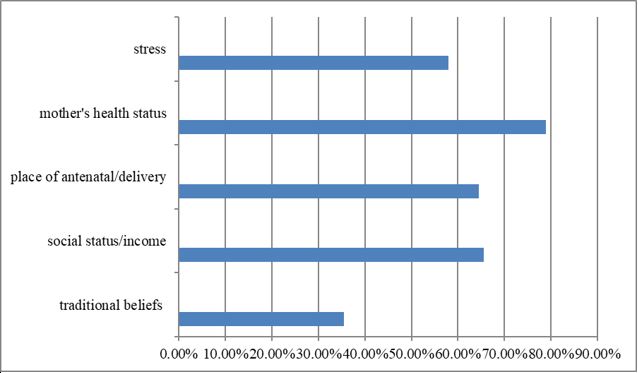
The postnatal mothers in the chart above identified the factors influencing their newborn care competence (efficacy and satisfaction) as traditional beliefs (N=27, 35.5%), social status/income (N=50, 65.5%), place of antenatal/delivery (N=49, 64.5%), mother’s health status (N=60, 78.9%) and stress (N=44, 57.9%).
P<0.05 level of significance
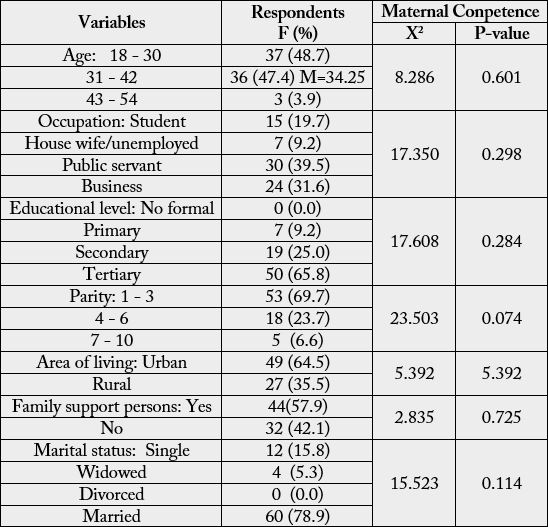
The table above shows the mean age of 34.25. Most of the mothers are in the 18 - 30 age brackets (48.7%), public servants (39.5%), tertiary education (65.8%), 1 - 3 for parity (69.7%), living in urban area (64.5%), has family support (57.9%) and married (78.9%).
As illustrated in the above table, chi-square test results at df=2, the value of 8.286 with p-value as 0.601 for age, X2=17.350, P=0.298 for occupation, X2 =17.608, p=0.284 for educational level, X2 =23.503, p=0.074 for parity, X2 = 5.392, p=0.370 for area of living, X2 =2.835, p=0.725 for family support persons and X2 =15.523, p=0.114 for marital status.
Discussion
The aim of this study was to determine the level of maternal competence of postnatal mothers regarding
new born care, identifying the factors influencing their competence level and examine the relationship
between maternal competence and the selected socio-demographic variables.
1. The respondents had high efficacy but low satisfaction. This shows that the mothers are not satisfied with the care they render to their newborn.
This is evidenced by the statements of most mothers, “sometimes I feel like I’m not getting anything done”, “Being a mother makes me tense and anxious”. “Even though being a mother could be rewarding, I am frustrated now while my child is at her present age”.
This result is consistent with that of the study of Emmanuel et al (2017) [3] and Shrooti et al (2016) [19]. The high efficacy level may be because more than half of the mothers (57.9%) have family support persons who are helping them with their role and care for the new born. This is in accordance with the study finding by Tarkku, (2003) [15] and warren (2005) [16]. Social support from family and friends can have a considerable influence on how mothers view themselves and in the care of their infants. Thus with increase in the number of persons present for assistance in infant care, the maternal role competence increased [10]. Social support can also be gotten from the midwifery and nursing professionals [17].
2. Postnatal mothers identified some factors which influenced their level of maternal competence.
Mother’s health status had the highest number of mothers which was followed by social status / income and place of antenatal / delivery. Stress was identified by more than half of the mothers while traditional beliefs had the least. These factors have been seen as having directly or indirectly influenced their level of maternal competence. According to Mercer (2006), Cultural and societal factors that may affect maternal competence on care of the new born include beliefs and traditions surrounding child bearing, social status and larger health care system [18]. Previous study by Paris, Bolton and Spielmen (2010) illustrated that maternal well-being such as depression, stress and anxiety contributed significantly to the level of maternal competence [19]. Concerning stress, Ngai and Chan (2012) suggested that mothers who experienced fewer stressors were mere likely to feel competent and satisfied in the maternal role during postnatal period [20].
3. Relationship was not established between the level of maternal competence and the socio-demographic variables (age, occupation, educational level, area of living, family support, parity and marital status) of these postnatal mothers. Similar findings were seen in the studies done by Ngai and Chan (2012) [20], Mercer and Ferketich (1995) [21] for parity and Emmanuel et al (2017) concerning occupation, education and family support [8]. Some previous studies have also shown contrary findings that family support [22] parity [23], significantly contributed to the level of maternal competence in new born care [24].
Conclusions
Focusing on the following of this present study, maternal competence level of satisfaction is low among the
postnatal mothers. It is of great importance to educate mothers on new born care from ante natal period to
enable them acquire the skills and become competent before delivery to facilitate positive adjustment and
satisfaction with maternal role.
Traditional beliefs, social status/income, place of antenatal/ delivery, mother’s health status and stress were identified as having influence on maternal competence level. However, no broad generalized because of the sample size and short period of study.
Recommendations
1. Essential new born care should be part of antenatal education programme.
2. Health promotion campaign should involve elimination of harmful traditional beliefs and practices, stress management / effective coping strategies, available social support groups and adequate health facilities with antenatal/delivery care services. These will enable us achieve improved maternal competence and UN-SDG3.
3. A repeat study on this topic should be done to include family support persons and health professionals.
Acknowledgment
We remain grateful to the Staff of Imo state Specialist Hospital Owerri and the postnatal mothers for their
support.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!