Biography
Interests
Gilbert Siu1*, Emily Cahalan2 & Todd Mingin3
1Department of Rehabilitation Medicine, Rowan University School of Osteopathic Medicine, Encompass Health
Rehabilitation Hospital of Vineland, USA
2ARC Seminars, USA
3Department of Physical Medicine and Rehabilitation, Virginia Commonwealth University, USA
*Correspondence to: Dr. Gilbert Siu, Department of Rehabilitation Medicine, Rowan University School of Osteopathic Medicine, Encompass Health Rehabilitation Hospital of Vineland, USA.
Copyright © 2020 Gilbert Siu, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Recurrent hemarthrosis in the knee joint is an uncommon disorder, often seen in the elderly population with severe knee osteoarthritis. Once diagnosed, the hemarthrosis can be treated conservatively with rest and pain medications, or invasively with joint aspiration or surgery. This case report describes the use of short stretch compression bandaging for the treatment of knee hemarthrosis. The application of short stretch compression wrapping as a therapeutic approach for this condition has never been documented. This is the first reported case, to our knowledge, of using short stretch compression therapy as a treatment for knee hemarthrosis.
Introduction
Elderly patients are at an increased risk for the rare condition of nontraumatic, spontaneous, recurrent
hemarthrosis of the knee. The broad differential should include other rare diseases such invasive malignancy, leukemia, crystal induced arthropathy, or idiopathic intra-articular hemorrhage [1,2]. In the absence of
suspicion for these conditions, mechanical factors in addition to increased vascular fragility may be the most
likely cause [1,3,4]. Mechanical risk factors for this condition may include severe knee osteoarthritis, lateral
greater than medial, with degeneration of the lateral meniscus [3,4]. Medical comorbidities contributing to
vascular fragility include hypertension, arteriosclerosis, and/or a hematological abnormality [1,3,4].
The etiological theories for this condition have evolved, initially with Wilson in 1959 indicating patellofemoral osteoarthritis with a fringe synovial source [5]. In 1994, Kawamura demonstrated early evidence for disruption of meniscal branches of the lateral geniculate artery within the posterior horn of the lateral meniscus to be a more likely causal factor [3,6]. This latter theory has continued to develop with additional literature, and is the currently recognized origin [6]. Even with the dominance of medial joint OA and medial meniscal degeneration, lateral joint degenerative changes more often are present with spontaneous recurrent hemarthrosis [1,4]. Anatomical analysis supports possible explanations for the bleeding from lateral meniscal origins, more so than medial [1,4]. Lateral and middle genicular arteries that supply the lateral meniscus are both closer to the meniscal rim, and are larger than the medial genicular artery [4,7]. Additionally, arthroscopic cases have demonstrated throbbing bleeding from this location during surgical procedures without using a tourniquet [3,4,6]. Effective surgical interventions such as lateral genicular arterial embolization, lateral meniscectomy, and electrocauterization have all been demonstrated successfully in the literature [1,3-5,8].
Initial attempt should be made to manage this condition conservatively, but understandably, surgical intervention may be required. In this case report, we present an additional conservative management option utilizing short-stretch compression wrapping. Short-stretch compression wrapping is a treatment using nonelastic, resistive, non-compressive forces, which are often used in the treatment of peripheral lymphedema.
Case Description
A 76-year-old right handed female with past medical history of severe right knee osteoarthritis presented
with worsening right knee pain and edema to the emergency room. On physical examination, the patient
demonstrated pain (10/10 on visual analog scale) with standing on the right leg, and pain with knee range
of motion (ROM). The patient’s knee flexion ROM was 0-10 degrees. The patient also had positive crepitus
at the right knee with noted joint effusion. Magnetic resonance imaging (MRI) of the knee was noted to be
positive for knee hemarthrosis. Patient had received three right knee intra-articular aspirations within the
past year by her orthopedic surgeon, without improvement in knee pain or mobility of her recurrent knee
hemarthrosis. Tramadol for pain relief was trialed with minimal effect. Due to the patient’s severe knee pain,
the patient’s initial functional status was Moderate Assistance for ambulation and activities of daily living
(ADL).
The patient was then transferred to inpatient rehabilitation hospital and an alternate approach to her recurrent knee hemarthrosis was initiated. Short stretch compression bandaging from toe to thigh high level of her right leg commenced (Figure 1). Compression wrapping continued for 10 days, along with other traditional therapies consisting physical and occupational therapies. During her treatment stay, the patient’s pain improved to 0/10 on visual analog scale, without oral analgesia; knee ROM increased to 0-90 degrees; and edema in the right knee decreased significantly. Ultimately, she progressed to Modified-Independent level in ambulation and ADL, and was discharged home with continued home short stretch compression wrapping of her right leg by home therapy.

Discussion
Recurrent knee hemarthrosis is an uncommon disorder in the elderly population. With the elderly population
increasing, the prevalence of knee hemarthrosis related to the aging vasculature of the joint is rising. The
etiology of these spontaneous hemarthroses of the knees have been documented to be from repetitive trauma to the synovium; menisci injuries; anticoagulation medications; complications from total knee replacements;
and aging of the knee peripheral vasculature [6,9]. The presence of the hemarthrosis causes acute pain and
swelling, ultimately impacting the patient’s functional status. Functional decline from the knee hemarthrosis
can further exacerbate the patient’s existing medical co-morbidities, and also cause other medical issues,
such as pressure ulcers, deep vein thrombosis, opioid dependence, depression, and infection. The first line
of treatment generally involves long-stretch bandages (ACE wrapping), ice, rest, and joint aspiration.
The success of these conservative treatments has been reported at ~30% [10]. When these treatments are
unsuccessful, surgical intervention is performed. Some of these surgical interventions include meniscectomy,
embolization of the arteries, and radiosynovectomy [10].
In this case, the patient has had multiple spontaneous recurrent hemarthrosis, owing to her severe knee osteoarthritis which was causing repetitive trauma to the knee joint. The patient had failed multiple conservative therapies, thus we started on alternative approach for the management of her knee hemarthrosis: short-stretch compression bandaging.
Compression therapy has been shown to have multiple effects in the orthopedic population: (1) increases pressure in the tissue, blood and lymph vessels; (2) improves venous and lymphatic return; (3) reduces net filtration; (4) improves the effectiveness of the muscle and joint pumping during activity; (5) breaks up and softens deposits of connective and scar tissue; and (6) provides support for tissues that have lost elasticity [11].
The addition of this treatment modality can improve healing by: decreasing the knee edema caused by the hemarthrosis; improving congestion of inflammatory lymphatic fluid and improving absorption (net filtration); and improving lymphatic circulation by harnessing muscle and joint pump action.
The inflammatory response experienced within the tissue of the knee joint as a result of hemarthrosis causes congestion and localized edema. This excessive accumulation of fluid is detrimental to healing owing to an increase in diffusion distance for oxygen and other nutrients, thereby compromising cellular metabolism and arresting the healing process. Similarly, the obstruction of lymphatic and circulatory pathways secondary to inflammatory edema will limit the removal of toxic byproducts of cellular metabolism [12]. It may therefore be surmised that by addressing the local edema and increasing lymphatic and circulatory drainage, the hemarthrosis may be absorbed more efficiently.
As compression bandaging also has the noted effect of increasing lymphatic circulation throughout the limb, by providing a resistive force to the skin which enables lymph vessels to open and allow fluid from interstitia and travel up lymphatic pathways. The efficiency of deeper lymphatic pathways are targeted through the combination of resistive compression and muscle activity, thereby improving the pain and decreased ROM related to the recurrent edema [11].
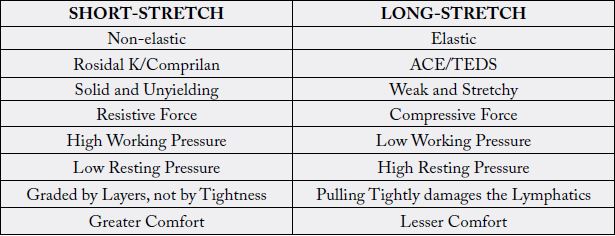
Compression bandages can be short-stretch or long-stretch (Table 1) [11]. The use of short-stretch compression bandages provides compression benefits, as those mentioned, above along with providing high working pressure and a low resting pressure. Short-stretch compression bandages are textile-elastic interwoven fibers that allows ~60% extensibility; whereas long-stretch bandages (i.e. ACE bandages) are polyurethane and allows ~140% extensibility, resulting in low working pressure, tourniquet effects, and constricting veins and lymph vessels [11].
The application of short stretch compression wrapping as a therapeutic approach for recurrent knee hemarthrosis, to our knowledge, has never been documented. Short stretch compression therapy improved our patient’s pain, edema and functional status. This is the first reported case of using short stretch compression therapy as a treatment for knee hemarthrosis.
Conclusion
Although recurrent knee hemarthrosis is rare, this disorder is becoming more prevalent owing to the rising
elderly population, and the complications that advancing age may present to the vasculature of the knee
joint. This case highlights the importance and the benefits of utilizing a non-invasive approach for treating
this condition, with an inexpensive and effective outcome. We believe that if included as a routine part of
rehabilitation, the orthopedic population will enjoy greater outcomes, and decreased ongoing complications.
Disclosures
Financial disclosure statements have been obtained, and no conflicts of interest have been reported by the
authors or by any individuals in control of the content of this article.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!