Biography
Interests
Sergio Luiz Carlos Dos Santos1*, Vera Moreira de Andrade, L. A.2 & Nuria Rodriguez Avila3
1Department of Sport Sciences, Federal University of Greater Dourados, Brazil
2PhD Student in Nursing and Health at the University of Barcelona, Professor at the School of Public Health,
Curitiba, Paraná
3Professor at the Post Graduation in Sociology and Health and Foreign Relations Vececana, University of Barcelona,
Spain
*Correspondence to: Dr. Sergio Luiz Carlos Dos Santos, Department of Sport Sciences, Federal University of Greater Dourados, Brazil.
Copyright © 2019 Dr. Sergio Luiz Carlos Dos Santos, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
The article presents systematic review of the health care environment, with emphasis on the profile of culture in hospitals. The method was searched in the databases PubMed, Embase and Scholar. Using the keywords assessment (and) culture of patient safety (and), hospitals, Judo athlete’s knee surgery, selecting publications between 2006 and 2015 and did not address reviews. Including only dealing with results with various professional categories under hospital safety culture. The languages for the articles were: English, Spanish and Portuguese. From this methodology it was possible to elect a total of 167 articles, 14 of which were chosen for the study, which resulted that the majority found a safety profile in the hospitals are influenced by the local culture tending mostly to positive. The limitations go through the lack of neutrality in the analysis even working in pairs and staff and research recommendations.
Resumen
El artículo presenta una revisión sistemática del entorno de atención médica, con énfasis en el perfil de la
cultura en los hospitales. El método se buscó en las bases de datos PubMed, Embase y Scholar. Utilizando la
evaluación de palabras clave (y) la cultura de la seguridad del paciente (y), los hospitales, la cirugía de rodilla
de atleta de judo, seleccionando publicaciones entre 2006 y 2015 y no se abordaron las revisiones. Incluyendo
solo tratar los resultados con varias categorías profesionales bajo la cultura de seguridad del hospital. Los
idiomas para los artículos fueron: inglés, español y portugués. De esta metodología, fue posible elegir un
total de 167 artículos, 14 de los cuales fueron seleccionados para el estudio, lo que resultó en que la mayoría
encontró un perfil de seguridad en los hospitales que está influenciado por la cultura local que tiende a ser
positiva. Las limitaciones pasan por la falta de neutralidad en el análisis, incluso trabajando en parejas y en
el personal y las recomendaciones de investigación.
Palabras Clave: Paciente; Seguridad; Cultura; Cirugía de Rodilla de Deportista
Introduction
Safety culture is understood as a product of values, perceptions, competencies, group and individual, that
determine a pattern of behavior and commitment to the management of safety [1] Through this attribute it
is possible to offer a safe assistance to the patient.
In the field of health care, patient safety has been gaining prominence and arousing interest from managers, health professionals and family members. In 2000, in the USA, the Institute of Medicine (IOM) article Err is human: building a safer health system was published in 2004, the World Health Organization (WHO) launched the World Alliance for Patient safety [2] which aims to promote patient safety globally. The first point of this document was directed to the education of health workers, especially the importance of hand washing before procedures. The second challenge is associated with reduced complications in surgeries and also verify the safety culture for patients athletes who underwent knee surgery and their care with the problem of falls. In Brazil, the National Program for Patient Safety (PNSP), established by Administrative Rule GM / MS No. 529/2013, aims to contribute to the qualification of health care in all health facilities in the national territory [3].
Numerous studies in several countries have shown the repercussions of the patient’s safety culture in the hospital environment. Faced with negative culture Factors such as job satisfaction, team work [4-6]. Reports of medical errors and incidents and the approach with which these medical errors and incidents are treated [7-9] levels of mutual trust, [9] stress level [4] are factors that generally affect the patient’s safety climate and consequently, make the patient’s safety culture positive or negative team leaders try to intervene in the workplace to avoid the factors that most contribute to the harm done to patients. The main causes reported in the literature are: fear of reporting errors, dissatisfaction with the profession and work overload.
To evaluate the safety culture of the patient, evaluation instruments were found among them the HSOPSC of the Agency for Healthcare Research and Quality-AHRQ [10] used in several countries. This research instrument has a version in many countries, including Brazil. Given this scenario, it is notable that a hospital environment with a positive safety culture and interventions to reduce adverse events brings benefits to the patient, family members, work team and the institution itself. Thus, this review aims to raise what the literature in the search on the subject to contribute to the scientific production on the topic and is justified to better understand the results of research on patient safety culture among researchers.
Judo is considered to be a highly accessible sport for different types of people independent of biotypes, genres and ages of people, although it does not have strong actions in its techniques, it is still one of the sports with a high rate of injuries CARAZZATO, CABRITA CASTROPIL, 1996 [11]. In this study, a group of patients who had been diagnosed as having traumatic injuries, or who had suffered injury and knee surgery, had been found to be “external” and / or external, 2013).
Goals
Objective will be to answer the question: What would be the profile of the evaluation on the culture of
patient safety in hospitals?
Through the literature review, this article aimed to raise the profile and how to evaluate the patient safety culture in hospitals selected in the articles meeting the criteria of the method, using the check list [12] presenting the participants, interventions, countries, comparisons and results, contributing with scientific production.
Methodology
The study of systematic review according to project registered in Prospero with number 420160198577. It is
an exploratory descriptive study through a bibliographic survey. A search was performed on 05/23/2016, in
the databases on available articles PubMed, Embase, Google Scholar using as keywords: assessment (and)
culture of patient safety (and), hospitals, Judo, lesions in athletes, Olympic wrestling, and Martial arts. The
languages for the articles were: Spanish, Portuguese and English. Duplicate articles and case reports were
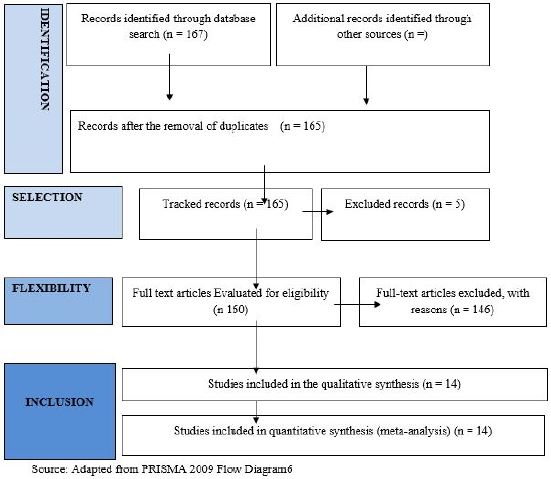
excluded. The order of selection of the articles is illustrated in the flowchart below, selecting publications
between 2006 and 2015.
Only articles in the full version were selected that met the study objectives and did not address reviews. The exclusion criteria were those that were not hospitals and out of the search object. Inclusion criteria are researches with several categories of health workers. Of the total of 167 articles found in the search, two were repeated. The distribution was as follows: 8 articles from Embase, five articles in the Google Scholar base and 153 articles in the PubMed database. The title role was organized into Excel R spreadsheets to analyze the inclusion and exclusion criteria. As inclusion, the articles that dealt with evaluation of the safety culture of the patient in hospital were determined; the others were treated as excluded. It started with the reading of the titles, beginning the elimination of the [13] duplications and [10] because they were revisions. The analysis was always in pairs and excluded 94 articles by the titles, [11] excluded in the readings of the abstracts and passing to floating reading of the complete articles accompanied by a reviewer finishing excluding another 26 articles because they were not meeting the object of the search. He then applied the filter choosing the focus of the theme of the proposed revision, leaving 14 articles that dealt with the evaluation about the safety culture of the patient. The following demonstrates the selection process:
Results
The 14 articles chosen by the pairs were analyzed grouped by results and groups such as from countries like China, Japan, Canada, Scotland, Belgium, the Netherlands, the United Kingdom, Lebanon, Saudi Arabia and the United States, and Brazil, concentrated in the years 2011 to 2013.
Among the selected articles we found studies using the SAQ-attitudes questionnaire that evaluated the employees’ attitudes regarding weak or strong aspects of the work climate on the safety of patients in health organization and HSOPSC as an example. The main objective of the research that evaluates the culture in the work environment is to identify these elements to enable an intervention and improvement in the hospital scope. There are numerous factors that contribute to a negative safety profile in hospitals. In addition, recognition of conditions that contribute to a positive profile is essential for maintaining those aspects that do not require change and need to be valued. We selected articles to evaluate the safety profile of the patient. There was great agreement between the aspects that lead to a positive or negative profile.
A positive safety climate brings great benefits to patients [4]. The essential elements for this climate are: the harmony of teamwork, individual satisfaction in the profession, recognition of stress and good job conditions. In this context, an analysis showed that improvement orientation, passion for mission / profession, prioritization of resource allocation and sharing of information in the team were significantly associated with a better realization of safety practices12 [7]. Already for all dimensions and also addressed in their analysis, the set that proved most effective for a positive profile was: feedback for learning in the face of error, teamwork and non-punitive response to professional failures.
On the other hand, the factors that imply a negative culture are always present in the hospital sphere, and most of the time they receive little attention to their management. The main factor for an ineffective safety culture profile was the lack of report of superior or responsible errors. Most of the time the absence of communication occurs for fear of punishment and even dismissal of employees. In addition, heavy workloads drastically affect the quality of patient safety, especially in hospitals schools. Another negative factor for the safety culture raised in the surveys was the non-anonymity for reporting errors. Several team members identify colleague failures, but do not feel safe to report events.
Local and local culture has a great influence on the patient’s safety climate. A study conducted in China and the US has proven this: Officials in Shanghai’s general public hospitals are much more likely to report their fear of shame (41.2%) than those in US hospitals (4.8%), this is because Chinese society tends to be more collective than Western society, which is called “family collectivism,” so to err means to shame the whole community.
In the face of the interpretations, there is a real need for short- and long-term initiatives to improve patient safety culture and provide each hospital with a baseline patient safety culture profile to direct an intervention plan. In addition, further research is needed to understand the association between patient safety culture and clinical outcomes [5]. The following table presents the resulting articles among those elected for this review:
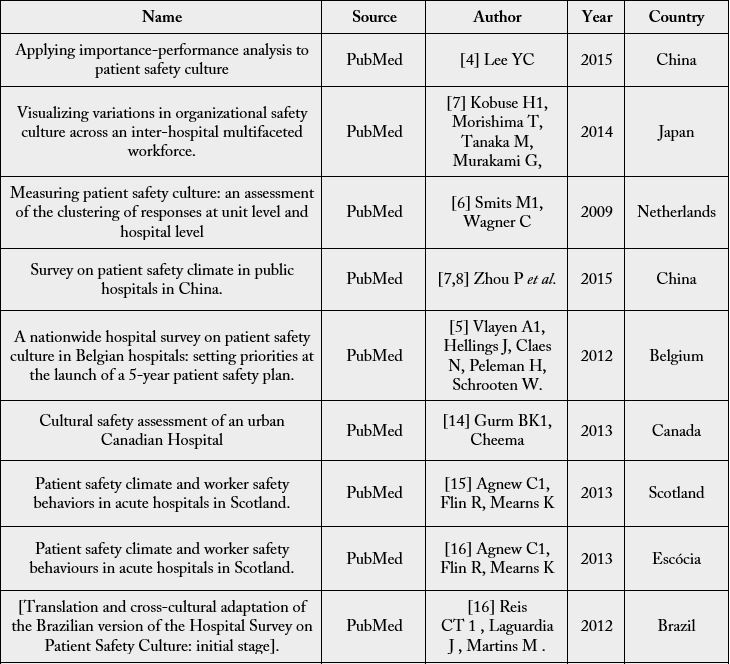
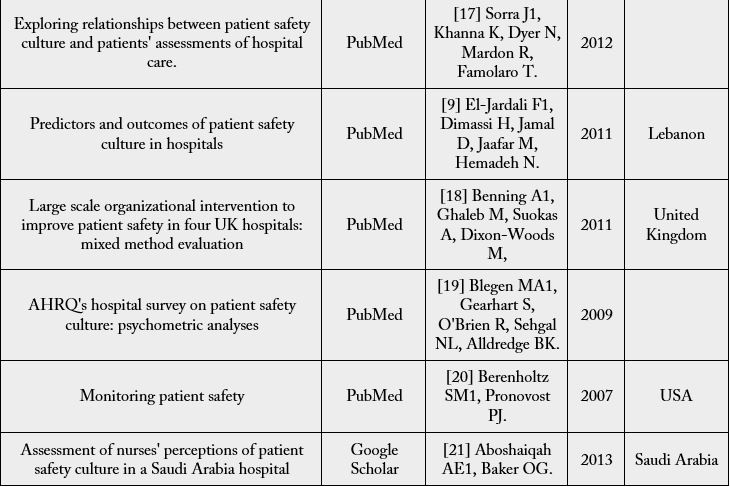
Source: Adapted by the authors of this Review from the Bases researched.
Discussion
According to the studies and articles presented, it is evident the importance of the Patient Safety Culture as
a philosophy applicable in the hospital universe and in health facilities. The issue, of global merit, has been
considered and studied in several countries of the world, while organizations and researchers together seek to define the internal issues of organizations that relate directly to patient safety.
The main motivators of the quest for a patient safety culture are the well-being of patients and their good relationship with the physicians and other staff who serve them. In order to effectively establish a robust patient safety culture, it is indispensable to the body of professionals involved the daily commitment to meet certain values, behavior patterns and attitudes established for this purpose [8]. It is noted, therefore, that not only individual efforts on the part of managers and staff, but a joint effort of the health organization as a whole, are necessary in order for such efforts to reflect on real and measurable results that actually positively affect patient safety [6-8]. Despite its great importance, only the isolated implementation of initiatives, actions and values of the patient safety culture is not enough. Culture itself is not measurable. In this way, the safety culture management and the measurement of the instant reality of patient safety in the organization’s environment play a fundamental role. The existence and “health” of the patient’s safety culture in an organization are corroborated through the patient’s safety climate analysis, which is performed through specific tools and questionnaires that generate indicators that are easier to interpret [7,8].
The studies of articles presented were good examples of the use of these tools. In these studies, Patient Safety Climate surveys were conducted in different countries (see Table 1), in different types of organizationacute hospitals, long-care hospitals, psychiatric units, etc., [5] covering different types of employees (doctors, nurses, pharmacists, laboratory personnel, administrative staff, supervisors, managers, among others). Some surveys are more restricted to certain types of staff, such as the evaluation of only doctors and nurses. Others, however, are more comprehensive, often including clerical staff and non-clinical staff [8,9].
These studies not only exemplify the conversion of the subjectivity of the patient safety culture into the objectivity of real and measurable indicators, but also indicate that these tools are applicable to different realities, environments and professionals. In other words, such tools allow to obtain patient safety climate measurements from diverse points of view, in different places. It is often necessary to develop new research instruments or new versions of existing research instruments [8]. In the cases studied, different research instruments were cited.
This cultural difference in the way of seeing the aspects that make up the patient’s safety is described in article 14 [8]. The study was conducted in China and US two countries with quite distinct cultures. In China, the physician-patient relationship was more conflicting and unsafe medical care was reported, and fear of guilt over an error indicated a greater barrier for the Chinese when compared to the Americans.
Regarding the research tools to raise the culture of patient safety cited is the HSOPSC, developed by the American Agency for Research and Quality in Health, second [8] is efficient in the USA but not very well administered in the context of its study in Shanghai. Nevertheless, it is the most widely used tool in hospitals in different countries20 [9].
Researches in hospitals in the USA22 [19], Lebanon20 [20], Belgium15, The Netherlands13 used this questionnaire and its variations. In Brazil the cross-cultural adaptation of HSOPSC. of ARQH. was made by Reis et al. Another research tool worth mentioning is the PSCHO, a research tool developed to evaluate the patient safety climate in US hospital organizations, but adopted in a version adapted to be applied in Chinese organizations. These modifications, as reported, would not only leave the questioned Chinese officials more comfortable answering the questions more accurately, but also sought to put their questions in a collective context rather than focusing on the individual14 [8]. Other more specific research instruments are mentioned, such as the SAQ-Safety Questionnaire mentioned in article 11, the Scottish Hospital Safety Questionnaire17 [15] and the SOPS Hospital [8,17] among others.
Patient safety surveys and surveys applied in each health organization allow us to relate the main factors that, from the point of view of those questioned, have a positive or negative impact on the patient’s safety climate[7,8]. Therefore, the variability of the questioned employees (gender, age, position, years of experience and the location (country, city, type of hospital organization, size, etc.) certainly influence the results of the surveys [21]). In each case specific results are raised with certain factors. What is seen is that some are more peculiar, while others are common to almost all cases studied, regardless of location. Factors such as job satisfaction, teamwork [4-6]. reports of medical errors and incidents and the approach with which these medical errors and incidents are treated [7-9] levels of mutual trust, [9] stress level [4] are factors that generally affect the patient’s safety climate and consequently, make the organization’s patient safety culture positive or negative.
From this, it is concluded that the culture of patient safety and its success, has a lot to do with the confidence and comfort that health professionals and other employees feel when performing their respective functions, and also with the capacity of the professional in deal with errors and incidents in your work environment. Patient safety should be a strategic priority for health organizations and their managers. There must be a system for identifying threats to patient safety, sharing information, and learning from events. In addition, there must be a collaborative environment so that all health care workers in the health organization can share and exchange information about patient safety [9]. The adoption of a collaborative, good communication and non-punitive culture is shown as a beneficial step along the way in the quest for patient safety, [6,8,9] an adequate flow of information, shared perception of the importance of safety, organizational learning and the commitment of management and leadership are issues that bring benefits in the culture of patient safety.
This identification of the main impact factors is essential because they are the basis for later action and initiative plans. These are the main issues and “problems” to be addressed, and this is where the greatest managerial effort must be concentrated. These actions should be taken at the most relevant organizational level according to Smits [6]. Usually they should occur preferably at the unit level rather than individual or hospital.
Finally, the results of the patient safety culture can be reflected externally to the organization. The results of the study by Sorra et al [17] showed a relationship of the success of the culture with the positive evaluation of hospital performance, fruits of good relations between employees and patients. Thus, not only patients with individual well-being, or employees and managers with a more adequate work environment and a friendlier relationship with the client, but also the hospital organization and its image before society are benefited.
Final Considerations
Concern about maintaining a positive patient safety culture has been a major challenge for hospital managers
around the world. This theme has gained more importance in the years, especially since 2004 with the World
Alliance for Patient Safety [2] program, created by the World Health Organization-WHO.
Through this systematic review it is evaluated that the safety profiles in the hospitals are influenced by the local culture. However, there is agreement among several points, among them: punishment of error lack of communication between staff, lack of academic preparation and poor working conditions contribute directly to a culture of negative patient safety. Among the most cited among those that lead to a quality of security are: orientation for improvement, passion for mission / profession, prioritization of resource allocation and sharing of information in the team.
The evaluation of culture and the identification of errors or negative factors many hospitals adopt measures to improve the scenario, such as: team training, learning by mistake, better material resources and incentives to work in a team. When these measures become effective, the patients the health team and even the family members are benefited.
This review is also important as a reference support of scientific production, including a thesis [22-26].
Limitations of the Review
The limitations of the study are the lack of neutrality of the eyes of each of the participating researchers, the
amount of search bases used in this research and the recognition and recommendation that other research is
necessary to approach more and better studies.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!