Biography
Interests
Alice Nguni1, Goma Fastone2 & Ravi Paul1*
1Department of Psychiatry, University of Zambia
2University of Leeds, United Kingdom
*Correspondence to: Dr. Ravi Paul, Department of Psychiatry, University of Zambia.
Copyright © 2019 Dr. Ravi Paul, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
The population of older adults with stroke in Zambia is rapidly growing and reports of cognitive impairments such as that caused by stroke are becoming more prevalent. Post stroke cognitive impairment is a common symptom of stroke and can have a significant effect upon a patient’s quality of life. In the case of a stroke, one or more cognitive domains may be affected, including attention, memory, language and orientation seem to improve among those who persist with Art therapy. Art therapy is a complex intervention capable of addressing the diverse impairment of post stroke patient. The present study investigated the evidence regarding the effectiveness of therapeutic Art therapy in improving Cognitive Functioning in older post stroke patients.
The objectives of the study were to 1) to evaluate how cognitive performance among post stroke
older adults improve significantly following 10 weeks of art therapy 2)to establish how Art therapy
attendance can positively be correlated with cognitive test scores (Clock Drawing Test and the
Cognitive Failures Questionnaire) and 3) to determine how cognitive performance outcomes scores for each of the two tests are correlated (the Clock Drawing Test (CDT) and the Cognitive Failures
Questionnaire (CFQ)).
The study utilized a Randomized controlled trial study comprising a sample of 72 participants
40(55.5%) females and 32(44.4%) males.
Perceived Clock Drawing test and Cognitive failure questionnaire were used to measure cognitive
functioning.
The study found out that the mean change in scores among interventional group members was
significantly greater than that of the control group (p< 0.05=.048 t=1.68, p=.048). There was
significant improvement of cognitive performance among interventional group members as
compared with the control group. Equally, the study found that Therapeutic Art therapy as a
treatment modality provided a medium effect size (d=.064).
Whilst available evidence is very limited, it suggests that art therapy may address many of the
diverse cognitive, emotional and functional needs of people disabled by stroke.
Introduction
Stroke is one of the primary causes of death and disability worldwide, [1] with a considerable proportion
of those having a stroke developing significant persistent cognitive deficits that impact on functional ability
[2]. Cognitive impairment has been reported in over half of patients 6 months post stroke and is associated
with increased disability and a poorer quality of life (QoL) [3]. There is limited but increasing research into
the benefits of creative arts therapies (including art, music, dance and movement, and drama) for people
living with various long-term physical conditions, but stroke has largely been neglected [2].
The prevalence of post- stroke cognitive impairment ranges from 20% to 80% [2], which varies for the difference between the countries, the races, and the diagnostic criteria. The risk of post-stroke cognitive impairment is related to both the demographic factors like age, education and occupation and vascular factors. The underlying mechanisms of post-stroke cognitive impairment are not known in detail. According to [3], it is estimated that 5% of all people over the age of 55 have evidence of cognitive impairments. There is evidence suggesting that the prevalence of cognitive decline after stroke would increase exponentially as age increases beyond 65 years [4]. Despite the prevalence of post stroke cognitive impairment, there is no established treatment aimed at improving cognitive function following a stroke.
The World Health Organization [5] defines stroke as the dysfunction of the brain due to a disturbance of cerebral blood flow. It is caused by interruption of the flow of blood to the brain (ischemic stroke) or the rupture of blood vessels in the brain (hemorrhagic Stroke). The interruption of blood flow or the rupture of blood vessels causes brain cells (neurons) in the affected area to die.
Therapeutic Art therapy “is a form of therapy which involves forms of expressive therapy that uses the creative process of making “art” to improve a person’s physical, mental and emotional wellbeing.” More also, it is a relatively new field, yet studies have shown overall improvement in patients who tried art therapy. The goal in Therapeutic Art therapy is for the patient to regain a sense of their ability to combine the physical motion with their thought. The field of therapeutic art therapy has been described as dynamic in both its delivery and treatment outcomes, and although the clinical practice of art therapy primarily deals with emotional expressivity, cognitive rehabilitation has been a documented goal with populations such as older adults [6,7].
In a related study by Musha, Kimura, Kaneko, Nishida, and Sekine (2000) [8,9], 41 Asian older adults were chosen out of a group of 118 experiencing cognitive impairment. They received one year of art therapy treatment. The researchers used EEGs during Art therapy to track changes in state of mind, such as mental stress, depression, joy, and relaxation, to see how the patients responded to the therapy. Joy was the most common response to the sessions. The study demonstrated that joy in Art therapy was associated with stabilization or improvement in cognition (as determined by MMSE scores) in 85% of participants.
Kenji et al. (2003) demonstrated that heightened emotion-based brain activity during Art therapy was correlated with enhanced cognitive performance, and Art therapy was associated with increased neuron activity (Kenji et al., 2003). Based on these findings, the researchers stated that future research was warranted on Art therapy as a preventative measure for dementia (Kenji et al., 2003).
Cognitive impairments affect about 80% of Stroke patients stoke statistic [9]. They are more common in the acute phase but many problems persist over time. The most common cognitive impairments among stroke survivors are memory, concentration, language and attention, executive dysfunction (initiation inhibition, mental flexibility) and aphasia [10].
Within this study, the term cognitive impairment refers to amnestic mild cognitive impairments (MCI). Language disturbance (for example, difficulty with sentence formation), attentional deficit (e.g., difficulty following conversations), and deterioration in visual-spatial skills (e.g., disorientation and an inability to appropriately utilize fine or gross motor skills) are all associated with amnestic MCI and were addressed within this study [11].
Researchers and clinicians have developed techniques for cognitive training programs to include puzzles, reading and verbal drills, and reasoning exercises [12]. Cognitive Training (CT) is beneficial in the improvement of cognitive performance (e.g., memory, concentration, and or coordination) and is a regimented therapy that usually takes place in a clinical or laboratory setting. Research shows that CT has improved cognitive abilities for up to five years following the initial training with up to 40% of individuals returning to normal cognitive functioning [13].
Cognitive impairments make patients have more severe deficits in activities of daily living, a worse functional outcome, more severe cognitive deficits and increased mortality as compared to stroke patient without depression. Therefore, to prevent cognitive dysfunctions of post stroke patients, psychological treatment should be recommended. Therapeutic Art therapy is one form of psychological therapy that can treat cognitive dysfunction and anxiety in stroke patients.
Therapeutic Art therapy integrates psychotherapeutic techniques with the creative process to improve mental health and well-being [14]. It is based on the belief that the creative process involved in artistic self-expression helps people to resolve conflicts and problems, develop interpersonal skills, manage behavior, reduce stress, increase self-esteem and self-awareness, and achieve insight. The use of Art therapy is limited, and as a result, outcome research on Art therapy with diverse older adults is lacking [15]. Previous Art therapy research on cognitive performance and older adults has been further limited by reliance on anecdotal evidence, non-randomized designs, and small sample sizes [16]. By using an a randomized controlled trial study design with a moderate sample size of older adults with stroke, this study sought to address this gap in research within the field of Art therapy by looking at the effectiveness of Art therapy in improving cognitive functioning among post stroke older adults.
This study carried out an investigation into the evidence regarding the effectiveness of Therapeutic Art therapy in improving cognitive functioning. In this regard, the study evaluated the effects of cognitive impairments on post-stroke older adults and further compared to how cognitive performance outcomes scores for each of the two tests are correlated (the Clock Drawing Test (CDT) and the Cognitive Failures Questionnaire (CFQ)).
Methodology
The study utilized a Randomized controlled trial study design. Controls and Intervention groups were
established through randomizing. A technique aimed at giving participants the opportunity to be assigned
to treatment conditions at random that is, they have an equal probability of being assigned to any group.
72 older adults with post-stoke (55-75 years old, average age=72.6, SD=5.9, the mean number of educational
years was 9.565, (range: 0-16 years), SD=2.91),) and had a history of stroke participated in this experiment
from outpatient clinic at the university teaching hospital. Exclusion criteria were: to be visually and or
Hearing impaired or has uncorrected deficits, Neurological and Psychiatric disorders, or difficulty executing
hand movements due to rheumatic diseases.
Participants were randomly assigned to two treatment groups. Treatment groups included Therapeutic Art therapy (intervention) which include (n=36) and the other treatment group was recreational group without Therapeutic Art therapy (controls) which included (n=36).
Before entry to the study all participants received an explanation on the objectives of the research, and signed an informed consent form. The Research Ethics Committee of ERES Converge approved this study.
In order to evaluate cognitive functioning, two tests were administered as pre- and post-intervention
evaluations: Clock Drawing Test (CDT) and Cognitive Failures Questionnaire (CFQ). The CFQ was
chosen because it was designed to assess elders who are experiencing cognitive impairments. It is a self
-report measures that has 12 subscales. Psychometric reliability and construct validity of the Cognitive
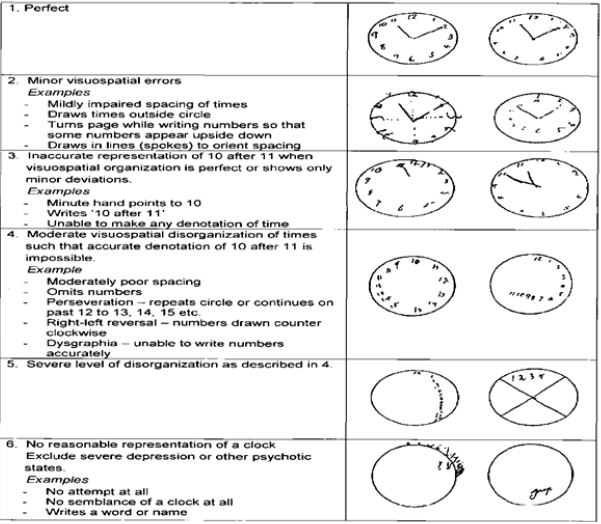
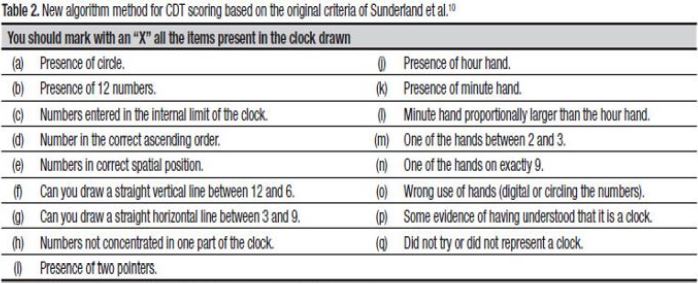
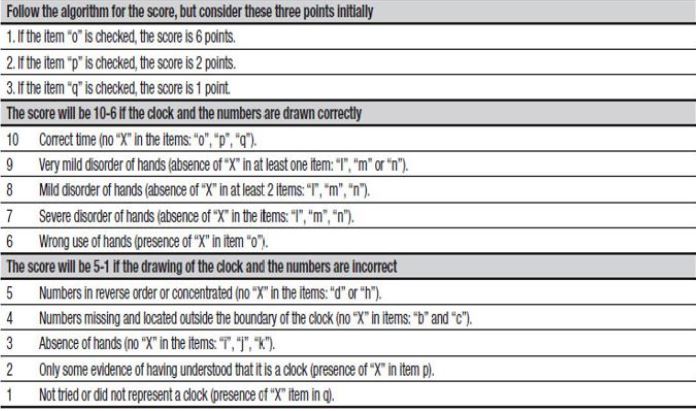
Failures Questionnaire (CFQ) have been established in many studies [17,18]. In addition, The Clock
Drawing Test (CDT) is an art-based neurological assessment that represents an objective measure of
cognitive performance.
Participants were first submitted to a standardized questionnaire, which collected data on socio-demographic
variables (i.e., gender, age and education), on subjective memory impairment (i.e., “Do you feel like your
memory has gotten worse? Absent minded or easily disturbed on one’s focused attention”).
The CDT was applied to all participants in the spontaneous modality that uses a pencil and blank sheet of paper. The patients were asked to draw a clock without a model. Trained therapist issued a standardized instruction: draw a clock, put in all number and set the hands to 10hrs:11min. There was no time limit. This measure was used because CDT meets the criteria for cognitive screening.
The therapeutic Art therapy was provided in Clinic 6. Five trained therapeutic Art therapist provided Art
therapy. Participants were randomly assigned to either the control or interventional group.
• Participants were randomly assigned to either the control (n=36) or interventional group (n=36).
• The interventional group was provided with Art therapy once a week for 10 weeks that included a
combination of expressive art-making, art education, learning about art materials, group socialization, and
reminiscence.
• The control group continued to be involved in recreational activities. Participants in the control group
socialized or not as they saw fit.
• Attendance was taken at every session. Following the 10 sessions, all participants were asked to complete
the CFQ for the second time.
Summary of Instruments used:
Results

C = control group; I = interventional group
On average, participants in the interventional groups frequently improved cognitive performance than control group for each of the two tests. The CDT scores were significantly higher within the interventional group (t=2.44, P=.017). The CFQ scores were higher but not significantly (t=.85, p=.40).
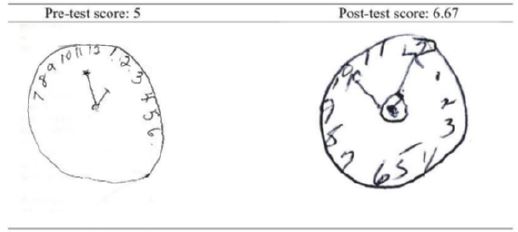
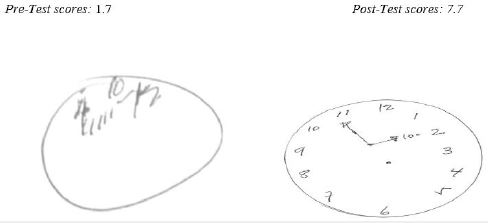
Above Figure (2 and 3) are examples of the CDTs from selected participants (A and B) who showed notable improvements. These clocks were chosen based on the clarity of improvement am the participants.
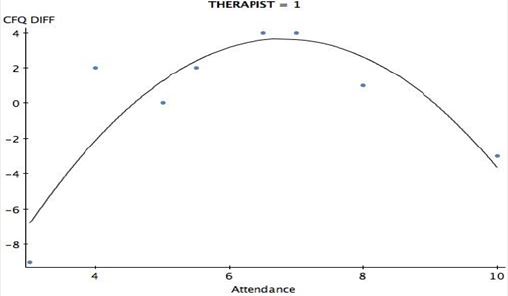
Attendance and performance scores were not significantly and positively correlated (CDT and attendance: r = -0.05; p = .697; CFQ and attendance: r = 0.05; p = .702).The results of the regression suggested that attendance affected cognitive performance optimally between 3 and 6 sessions.
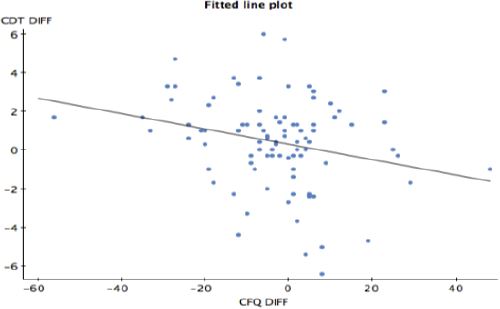
All participants in both the control and interventional groups, the findings suggested that the better the participants performed on the CDT, the worse they rated their memory on the CFQ subjective measure of cognitive functioning (r = -2.521; p = .013).
When the data were converted into a binomial variable, expressing 1 for improvement in score and 0 for a decline, the findings showed a distinct relationship (See Figure B).
Discussion
Demographics (age, education, medication use, level of functioning, attendance) all affected the outcome of
this study.
At pretest, the more educated an individual was, the higher his or her CDT score. The posttest yielded
different results, which related to the literature presented. For example, [19] found that, the brain responds
to enriched environmental input, which can modify the structure of the brain at any age and enhance
performance. Older adults improved significantly in cognitive performance despite lower education levels,
as 60 demonstrated by increased CDT scores at posttest. This contrast in education and improvement may
have contributed to the reason education was no longer significantly correlated with CDT scores at posttest
and why there was a negative correlation between CDT and education after the treatment.
When considering all group members, regardless of ethnicity, age was not found to be significantly correlated
with CDT pretest scores (r = -0.194; p = .0659). The CDT pretest scores were negatively and significantly
correlated to age among older adults (r = -0.408; p = .0224). At post-treatment, age was found to be negatively
correlated with improvements in CDT scores (r = -.209; p = .048). There was a positive correlation between
age and CFQ scores; however, this correlation was not significant (r = .191; p =.070).
In this study, more sessions did not necessarily yield better performance, but longer session duration and
combination approaches did. The correlation between therapy duration and CDT difference scores was
significant and positive (r =.555; p < .000); however, this correlation was not seen with CFQ scores (r =
-.153; p = .267).
Similarly, these results match other studies which positive significant scores in CDT unlike negative correlation among the CFQ scores According to summary statistics, therapeutic approach also affected CDT difference score: a combined art therapy approach, which incorporated both an art-as-therapy and art-psychotherapy approach, resulted in improved CDT scores (r = .568; p < .000), but not improved CFQ scores (r = -0.164; p = .236).
Within this study, when asked whether medication was taken for memory, many of respondents initially
answered yes and then explained that their doctor prescribed medication for their diabetes, blood pressure,
or other health concerns. Although these health concerns do increase the likelihood of declines in cognitive
performance, a prescription for blood pressure, for instance, would not be given by a doctor to treat cognitive
impairment.
These results of the present study seem to be consistent with other research findings have suggested that psychotropic medication is not a culturally compatible approach to treating ethnically diverse older adults [20]. One reason is that one third of minority patients read at or below the sixth grade level (i.e., low literacy), resulting in difficulty understanding prescription medication warning labels [16].
The results of the study provided evidence in support of the first hypothesis: older adults demonstrated
improvement in cognitive performance as a result of 10 weeks of art therapy. Both the t-test and the
univariate regression analyses yielded significant results for the CDT measure of objective cognitive
performance. This suggests that Art therapy provided cognitive performance benefits among older adults.
In addition, the results suggested that 10 weeks of Art therapy positively affected cognitive functioning but
did not positively affect self-perception of cognitive abilities. These results of the present study seem to be
consistent with other study findings in which [19] found out the attendance of Art therapy after more than
5 weeks sustained cognitive benefits ensured such as improved attention, sequences planning as shown by
the improving organization of images over the whole page and their more recognizable content.
The results of the regression suggested that attendance affected cognitive performance optimally between
3 and 6 sessions. The therapeutic approach, along with the duration of therapy, affected improvement in
cognitive performance more than frequency of attendance. In this study, more sessions did not necessarily
yield better performance, but longer session duration and combination approaches did.
The results of the study did not provide evidence in support of objective two. In support of this [20] authors observed that over time, coupled with other therapeutic arts experience lead to improvement in cognitive skills and language unlike attendance only.
Similarly, the results of this study paralleled the literature reviewed in which [21] assessed over time, the drawing revealed improvements in spatial awareness, symmetry and manipulation of shape. The client’s attention, memory and conceptualization are said to improve over time.
The results of the study provided evidence in support of the third hypothesis, which held that pre- and
posttest results would be correlated. Self-perception (CFQ) and cognitive ability (CDT) did show a correlation, though it was negative: participants with higher gains in cognitive performance reported that
their cognitive functioning had worsened. Considering all participants in both the control and interventional
groups, the findings suggested that the better the participants performed on the CDT, the worse they rated
their memory on the CFQ subjective measure of cognitive functioning (r = -2.521; p =.013). When the
data were converted into a binomial variable, expressing 1 for improvement in score and 0 for a decline, the
findings showed a distinct relationship (See Figure 15). The interventional group did not show significant
scores for a negative correlation (t = -1.556; p =.126); however, the analysis for the control group indicated
that the negative correlation was significant (t = -2.410; p = .021) [22-27].
Conclusion
The objective of this study was to evaluate the effectiveness of Art Therapy in improving Cognitive Function
in older Post- Stroke patients. Other outcomes included the findings that age, education, and independent
status all influenced participant responsiveness to art therapy as a treatment. The results suggested that Art
therapy may positively affect cognitive performance. Additionally the results suggested that Art therapy may
be culturally competent therapeutic approach.
Acknowledgement
To my dearest mother, I feel indebted to you for your painstaking help and support.
Disclosure
The authors declare no conflict of interest.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!