Biography
Interests
Shahram Mosharrafian, Mojgan Kargar*, Fateme Almasi & Mohammad Hassan Hamrah
Department of Pediatric Dentistry, School of Dentistry, Tehran University of Medical Sciences, Tehran, Iran
*Correspondence to: Dr. Mojgan Kargar, Department of Pediatric Dentistry, School of Dentistry, Tehran University of Medical Sciences, Tehran, Iran.
Copyright © 2020 Dr. Mojgan Kargar, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Dental trauma causing crown-root fracture is among the most challenging types of dental traumas in terms of management, which often involves maxillary permanent incisors prior to completion of their root development and can result in tooth loss. Management of this type of tooth fracture often requires a multidisciplinary approach with the cooperation of an endodontist, a periodontist, a pediatric dentist and/or an orthodontist. The primary goal of treatment in such patients should be preservation of the tooth and reinstatement of dental esthetics and function. This case report describes management of a challenging case of complex crown-root fracture of a maxillary central incisor in a 13-year-old boy, which was performed by endodontic treatment, orthodontic extrusion and crown lengthening surgery followed by post space preparation in the root canal and crown build-up with composite resin. The patient was followed up for 6 months in terms of periodontal health, esthetics and function, with satisfactory results.
Introduction
Crown-root fracture accounts for 5% of all dental traumas to permanent teeth, which often occurs due to
direct trauma to the anterior teeth. The fracture finish line often extends below the cementoenamel junction,
involving the enamel, dentin and cementum, with/without pulpal involvement [1]. The direction of fracture
line, size and mobility of the broken segment, subgingival extension of the fracture line, developmental stage
of the tooth, alveolar fracture, soft tissue injury, and dental pulp status can all affect the treatment outcome
[2]. Several treatment modalities have been suggested for management of crown-root fractures including
(I) removal of the broken segment and restorative treatment, (II) gingivectomy and osteotomy to expose
the fracture line and then restore the tooth, (III) orthodontic extrusion with/without gingivoplasty, (IV)
surgical extrusion, and (V) tooth extraction and prosthetic replacement [3,4]. Orthodontic extrusion is a
conservative treatment approach to expose the subgingival fracture line by forced eruption of the tooth.
It can also result in formation of attached gingiva and stable periodontal condition and can bring about
excellent esthetic results in most cases [1,5]. This case report describes successful management of crownroot fracture of a maxillary central incisor in a 13-year-old boy with orthodontic extrusion and appropriate
prosthetic and restorative treatments.
Case Report
Our patient was a 13-year-old boy presenting to the Pediatric Dentistry Department of School of Dentistry,
Tehran University of Medical Sciences complaining of fracture of his maxillary anterior teeth due to a fall
that had occurred one day earlier.
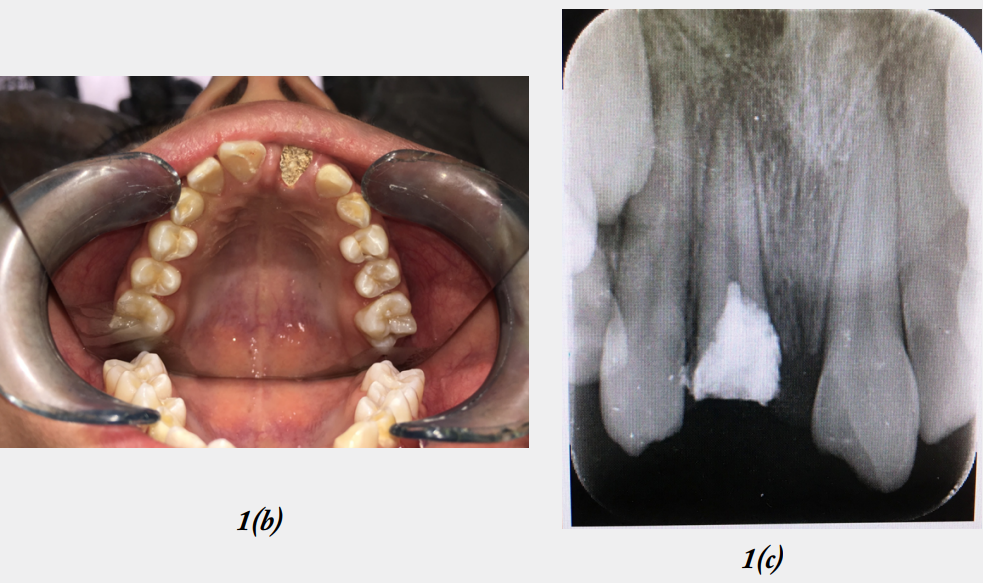
Clinical and radiographic examinations revealed complicated crown-root fracture of maxillary right central incisor causing pulp exposure. The fracture line had extended 2mm below the alveolar bone crest in the palatal surface. Also, the maxillary left central incisor had complicated crown fracture with pulp exposure, and the maxillary right lateral incisor had uncomplicated crown fracture (without pulp exposure). The patient had presented to a dental office 2 h after trauma (the day before) and the dentist had performed pulpotomy for the maxillary right central incisor and had temporarily restored the tooth with a cotton pellet and Zonalin (Figure 1).

We decided to perform Cvek pulpotomy for the maxillary left central incisor considering the small size of the mesial pulp horn exposure and the fact that only 24 hours had passed since trauma. This was done to allow completion and maturation of root. For this purpose, a high-speed handpiece and a diamond bur along with water coolant was used to amputate about 2mm of the pulp tissue. The area was then rinsed, and the hemorrhage was stopped. Next, the amputated pulp tissue was coated with mineral trioxide aggregate (MTA), a moist cotton pellet was placed over it, and the tooth was temporarily restored with light-cure glass ionomer. After 2 days, the temporary restoration was removed to ensure complete setting of the MTA. Next, glass ionomer was applied over the MTA, and the tooth was permanently restored with composite resin.
Regarding the maxillary right lateral incisor, since the pulp horn had not been exposed and the tooth responded normally to vitality tests, light-cure glass ionomer was applied over the site of dentin exposure to prevent further hypersensitivity prior to permanent restoration of the tooth. Due to the time shortage for final restoration of this tooth in the first session, its composite restoration was postponed to the second session.
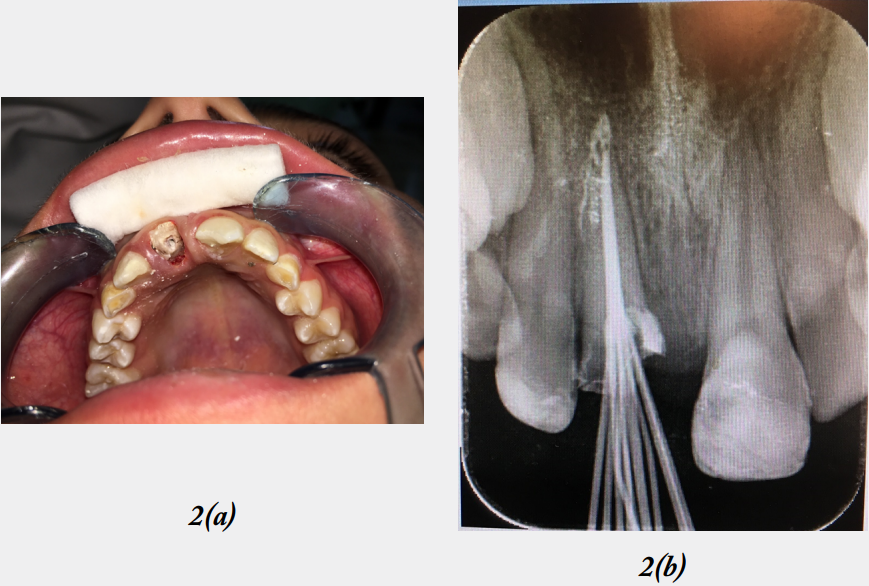
In the maxillary right central incisor, the fracture line was 2mm below the alveolar bone crest in the palatal side, which could complicate the restoration of the tooth and compromise the prognosis of treatment. Considering the significance of this tooth in the esthetic appearance of the patient, appropriate root length, favorable periodontal status, good oral hygiene of the patient and his enthusiasm to continue treatment, we decided to preserve the tooth by orthodontic extrusion to expose the fracture line supragingivally and enhance the restoration of the tooth. For this purpose, the respective tooth first underwent root canal therapy. A radiograph was obtained to determine the working length, and the root canal was instrumented to the working length in the first session. Calcium hydroxide was applied as intracanal medicament to prevent infection and the tooth was temporarily restored with Zonalin. After 2 weeks, calcium hydroxide was removed from the root canal, endodontic treatment was accomplished, and the tooth was temporarily restored with Zonalin (Figure 2).
For orthodontic extrusion, first an alginate impression was made and a removable appliance was fabricated, which included two Adams clasps, one modified labial bow, and one hook placed in the palatal vault of the appliance for attachment of elastics (Figure 3).

A small hole was created in the remaining tooth structure in the buccal surface of the tooth with a small round bur and high-speed handpiece. A double layer ligature wire was passed through the small hole and created a hook. After appliance delivery to the patient, one elastic was hooked to the ligature wire after passing through the more prominent part of the labial bow and connected to the palatal hook of the appliance. The elastic applied vertical load along the longitudinal axis of the central incisor root. Medium elastics with an inner lumen size of 3/16” were used and the patient wore the appliance at all times (except for when eating) (Figure 4).

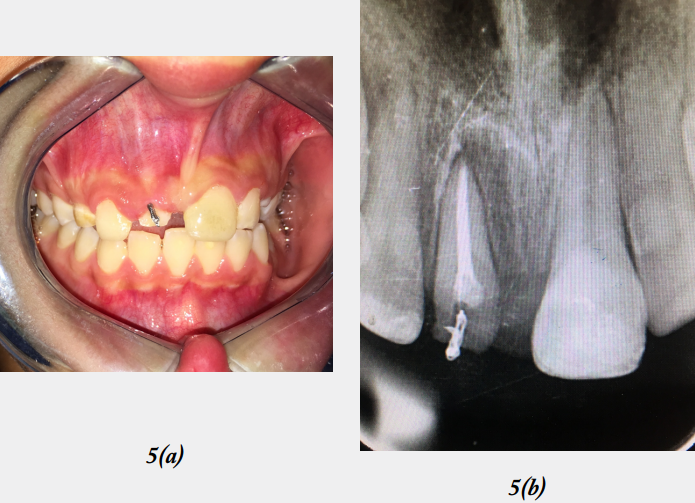
After 3 months, 4mm extrusion was achieved, which provided adequate tooth structure for restoration retention and an approximate crown/root ratio of 1:1. In order to stabilize the tooth position and decrease the risk of relapse, the tooth was maintained in the retention phase by passive elastic force for 3 months (Figure 5). After the retention phase, the respective tooth underwent crown lengthening surgery to match the level of gingiva with the adjacent gingiva and provide optimal esthetics (Figure 6).

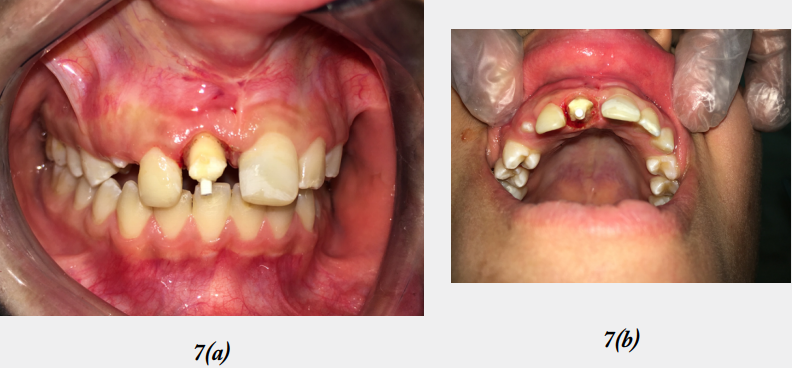
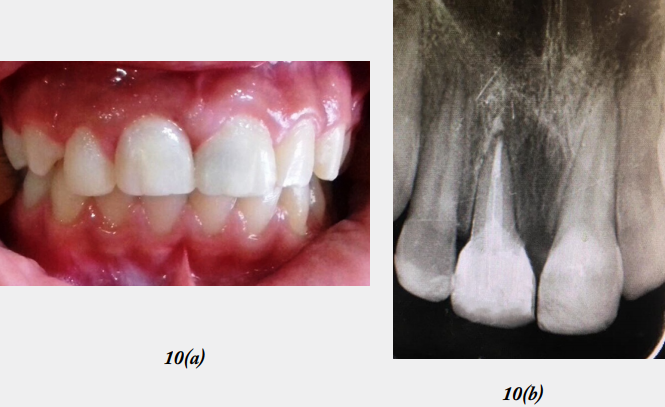
During the restoration session, the gingival tissue of the respective tooth was slightly formed by electrocautery to obtain optimal gingival margin contour. In order to provide adequate retention for the restoration and considering the young age of our patient, which did not allow metal post and core, and crown placement, we decided to place a fiber post in the root canal (Figure 7). The tooth was temporarily built up by composite resin until completion of alveolar bone growth and final restoration of the tooth (Figures 8 and 9). The tooth was followed-up for 6 months regarding periodontal health, esthetics, and function, with satisfactory results (Figure 10).



Discussion
Of the suggested treatment modalities for complex crown-root fractures, orthodontic extrusion is a
conservative approach that also preserves periodontal health and brings about excellent esthetic results in
most cases [1].
The speed of orthodontic extrusion may be rapid or slow. In rapid extrusion, the alveolar bone remains in place and does not erupt along with the tooth. In rapid extrusion, circumferential fiberotomy may be required after extrusion to prevent relapse [6]. The disadvantages of rapid extrusion include the risk of perforation of the periodontal ligament, ankylosis of the tooth, and risk of root resorption [7]. In slow extrusion, the alveolar bone and the gingival tissue move along with the tooth. In such cases, crown lengthening surgery may be required to expose adequate amount of tooth crown to allow for the ferrule effect, and provide a resistant and retentive form for the final restoration [6]. Slow extrusion occurs at an approximate speed of 1 mm or lower per week. It has been recommended that the maximum load applied to the root for slow extrusion should not exceed 30g while rapid extrusion is performed with loads > 50g [8]. Considering the optimal crown/root ratio of 1:1, a central incisor can be extruded by 2-4mm and a lateral incisor can be extruded by 4-6mm; although no study has cleared that in case of preserving a stable periodontal support, the crown/ root ratio of 1:1 cannot be exceeded [1].
Several methods have been described for orthodontic force application to the teeth. If the remaining tooth structure has a large surface, an orthodontic bracket should be bonded to the tooth [6]. If the entire crown is broken and only the root remains, forming a J hook by using a steel wire and its cementation to the root can help [9].
In our patient, a type of removable appliance was designed to connect the elastics and apply loads to the Tooth, which have not been used before for orthodontic extrusion. The designed removable appliance included Adams clasps on permanent first molars, a labial bow, and a hook in the palatal vault to attach the elastics. By reshaping the labial bow and its vertical distancing and approximation to the cervical region of the teeth, the elastic length could be adjusted to apply the desired load to the tooth.
A removable appliance has advantages such as easy fabrication, not requiring fixed orthodontic treatment, more general application, better acceptance by patients, and easy removal after treatment completion [10]. In our patient, instead of placing a hook in the root, a small hole was created in the remaining tooth structure in the buccal surface and a ligature wire was passed through the hole to create a hook, which was used for elastic attachment. This method was simple and practical, and eventually the created hole was filled with composite. The orthodontic traction force can be applied to the respective tooth by orthodontic elastics, elastic chains, looped wire or spring [8,9]. According to the manufacturers’ instructions, the elastics apply the magnitude of load written on their pack when they are stretched out by 3 times their diameter [11]. In order to prevent unfavorable root bending, the load should be applied along the longitudinal axis of the tooth [8]. Considering these principles, the forced eruption was commenced by medium elastics to achieve sufficient eruption of the tooth.
The main limitation of orthodontic extrusion is that it increases the duration of treatment and requires a long retention phase [12]. The retention phase after extrusion is 4 weeks for each 1 mm extrusion according to the literature. In our patient, a 3-month retention period was considered due to 3 mm of tooth eruption [8]. Considering the age of our patient and the fact that vertical growth of the face is not completed before the age of 19 years, and the possible alterations in the gingival margin and position of the tooth and esthetic compromise of the results of indirect restorations such as prosthetic crowns, we decided to place a fiber post in the root canal and restore the tooth with direct composite restoration [13].
Our patient showed optimal clinical and radiographic results and favorable esthetics and function during the 6-month follow-up, and the restoration is therefore expected to serve its purpose until 18 years of age or even longer. Regular follow-up sessions have been scheduled every 6 months for the patient to prevent complications and provide necessary interventions whenever required.
Conclusion
Orthodontic extrusion is a conservative treatment approach to expose the fracture line of a tooth, and has
several advantages such as favorable stability and excellent esthetic results. The position of fracture line
may prevent achieving adequate crown/root ratio and compromise the success of treatment to some extent.
However, in case of successful treatment, such teeth can be preserved at least until an appropriate time for
implant placement with optimal esthetic results.
Funding
This study did not receive any financial support.
Conflicts of Interests
All authors declare no conflicts of interest.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!