Biography
Interests
Khalid S. Aljabri1*, Samia A. Bokhari2, Nawaf K. Aljabri3 & Bandari K. Aljabri4
1Department of Medicine, Dr. Sulaiman Alhabib, AlKhobar, Kingdom of Saudi Arabia
2Department of Endocrinology, King Fahad Armed Forces Hospital, Jeddah, Kingdom of Saudi Arabia
3Department of Laboratory, King Fahad Armed Forces Hospital, Jeddah, Kingdom of Saudi Arabia
4College of Medicine, Um Al Qura University, Makkah, Kingdom of Saudi Arabia
*Correspondence to: Dr. Khalid S. Aljabri, Department of Medicine, Dr. Sulaiman Alhabib, AlKhobar, Kingdom of Saudi Arabia.
Copyright © 2020 Dr. Khalid S. Aljabri, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Overweight and obesity among women of childbearing age are important. We aim to evaluate the
frequency of overweight and obesity among Saudi women of childbearing age.
We conducted a cross section study to analyze female participants. A total of 5152 between the ages
15 to 49 years were selected to be enrolled for the present study between January 2018 to December
2019 at the Endocrinology Department of King Fahad Armed Forces Hospital, Jeddah, Saudi
Arabia. BMI values classified into groups as lean (BMI <18.5), normal weight (BMI=18.5 - 24.9
kg/m2), overweight (BMI=25.0 - 29.9kg/m2), obese Grade I (BMI=30 - 34.9kg/m2), obese Grade
II (BMI=35.0 - 39.9kg/m2) and morbidly obese (obese Grade III) (BMI≥40kg/m2).
The total sample size was 5152 women. Mean age was 36.6±9.0 years. BMI is skewed positively
(0.706). We found 145 (2.8%) were lean, 947 (18.7%) were normal weight, 1363 (27.0%) were
overweight, 1234 (24.4%) were obese Grade I, 830 (16.4%) were obese Grade II while 532 (10.5%)
were morbidly obese (obese Grade III). The frequency of overweight and obesity increased with
advance with age group and morbid obesity was highest in the 30 - 39 year age group. BMI are
skewed positively with each age group respectively. BMI showed an increase with advanced age, The
correlation coefficient (r) between age and BMI was r = 0.337, P<0.0001.
The frequency of overweight and obesity among women of childbearing age is high and considered
as a critical public health concern.
Introduction
For both the developing and developed nations, the increase in worldwide overweight and obesity rates was
a major public health epidemic [1]. Several risk factors could attribute to body weight including behavior,
environment, genes, metabolism and socioeconomic status [2-4]. Overweight and obesity are defined as
abnormal or excessive fat accumulation in the fat tissues of the body which are measured by a body mass
index (BMI) [5-7]. It is well established that obesity is associated with hypertension, diabetes mellitus and
cardiovascular disease [8].
Globally, about 30% of the world’s population are either overweight or obese [9-12]. In 2008, 35% of adults aged 20 plus were overweight (BMI > 25kg/m2), 35% were female where 28% of pregnant women are overweight and 11% are obese [13]. The highest rates of overweight and obesity were seen in the North Africa and Middle East in 2013, where more than (65%) of female age 20 or older were found to be either overweight or obese [10]. More than 600 million of adults, aged 18 years and older, were overweight in 2014 [11,12,14]. By 2015, 700 million adults worldwide will be obese as projected by the world health organization (WHO). Overweight and obesity affects female and male disproportionately between developed and developing countries. In 2014, WHO found that about (40%) and (15%) of female in developing countries were either overweight or obese respectively [14-17]. Worldwide, the proportion of women who are obese is higher than that of male (40% vs. 38%).
The prevalence of obesity and overweight in Saudi Arabia has been reported to be high in Saudi females [18-25]. Research indicates that a woman who is overweight or obese before she becomes pregnant also has a higher risk of complications during her pregnancy and higher prevalence of health problems for her children.
Women of childbearing age, defined by the WHO as women aged between 15 and 49 years 26. Since obesity increases the risk for several pregnancy complications and adverse maternal and fetal outcomes, prevention of obesity among women of childbearing age is crucial 27. We aim to evaluate the frequency of overweight and obesity in women of childbearing age in the western part of Saudi Arabia.
Methods
We conducted a cross section study to analyze female participants who are between the ages 15 to 49 years.
A total of 5152 were selected to be enrolled for the present study between January 2018 to December 2019
at the Endocrinology Department of King Fahad Armed Forces Hospital, Jeddah, Saudi Arabia. Pregnant
women were excluded. Weight (kg) and height (cm) were measured by nurses. BMI values classified into
groups as lean (BMI <18.5), normal weight (BMI=18.5 - 24.9kg/m2), overweight (BMI=25.0 - 29.9kg/m2),
obese Grade I (BMI=30 - 34.9kg/m2), obese Grade II (BMI=35.0 - 39.9kg/m2) and morbidly obese (obese
Grade III) (BMI≥40kg/m2) 28. The total number of females were separated on basis of age values into 4
groups: 15 – 19 years, 20 - 29 years, 30 - 39 years and 40 - 49 years.
Statistical Analysis
Univariate analysis of demographic and clinical laboratory was accomplished using unpaired t-test between
variables, to estimate the significance of different between groups where appropriate. Chi square (X2) test
were used for categorical data comparison. Pearson correlation was used for correlation between variables All
statistical analyses were performed using SPSS Version 23.0. The difference between groups was considered
significant when P<0.05.
Results
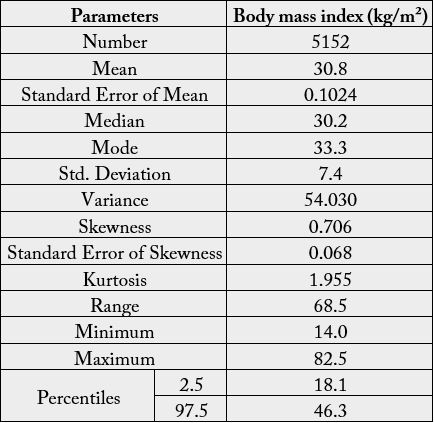
A total of 5152 women were analyzed. Mean age was 36.6±9.0 years. The median, mean, mode, standard
deviation, kurtosis and skewness of BMI in the Saudi females is presented in Table 1. Frequency distribution
histogram for BMI is presented in Figure 1. A normal Gaussian distribution is shown by the histogram.
BMI is skewed positively with a skewness of 0.706.

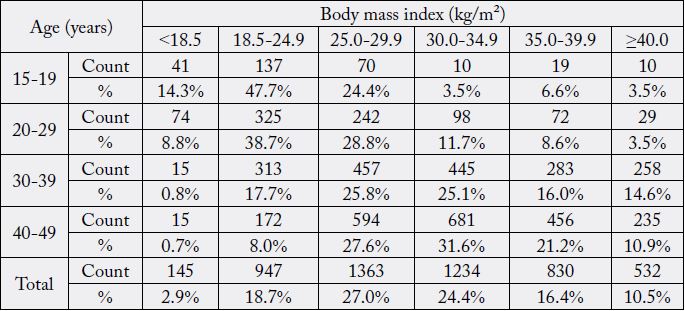
In the study population, 145 (2.8%) were lean, 947 (18.7%) were normal weight, 1363 (27.0%) were overweight, 1234 (24.4%) were obese Grade I, 830 (16.4%) were obese Grade II while 532 (10.5%) were morbidly obese (obese Grade III), Table 2. The frequency of overweight and obesity increased with advance with age group and morbid obesity was highest in the 30 - 39 year age group.
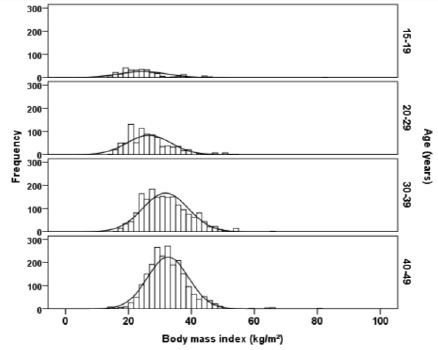
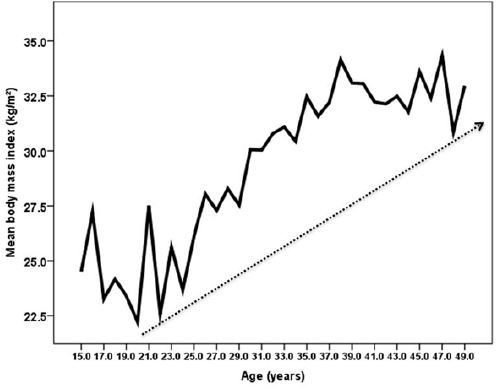
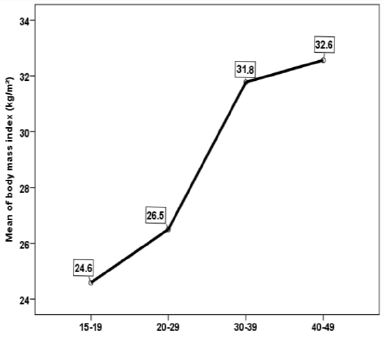
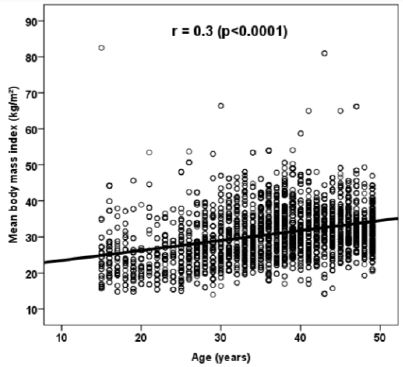
BMI within age groups are skewed positively with a skewness respectively for each age group, Figure 2. The results show that the values of the mean, median and mode are very close to each other suggesting normal Gaussian distribution as shown by the histograms. With an increase in age, BMI showed a gradual increase, Figure 3 and 4. The correlation coefficient (r) and P value between age and BMI was r = 0.337, P<0.0001, Figure 5.
Discussion
Worldwide, 30% of the world’s population are either overweight or obese [28]. Obesity is the most common
nutritional disorder in developed countries and is becoming significant in developing countries, and more
women in the fertile ages become overweight and obese. Obese women have higher risks of complications
during pregnancy [29,30]. Obesity in women of reproductive age was found in 25% of cases. In the United
States, obesity affects more than one third of the population and thus threatens the health of the nation
including diabetes, heart disease [31,32]. In 2014, WHO found that about 15% and 40% of women in
developing countries were either obese or overweight respectively [28]. In addition, the Health Survey
for England found that obesity increased in women from 16% in 1993 to 26% in 2011 [33]. obesity may
be regarded as an epidemic in Saudi adults like the developed countries of the world. Because of women’s
childbearing role, obesity in female has greater epidemiological importance than in male [34]. Females of
childbearing age are at especially high risk because of the increased health risks of pregnancy complications
and birth defects [35]. In our study, we randomly recruited adult Saudi females of childbearing age. We
demonstrated that the frequency distribution histogram of BMI shows normal Gaussian distribution with
skewness of 0.706 and kurtosis of 1.955. When the females are grouped into different age groups, an increase
in BMI found from 24.6±7.4 in the 15-19 y group to 32.6±6.5 in the 40-49 years age group. The correlation
coefficient is high and a statistically significant positive correlation between age and BMI is found (r = -
0.337, P<0.0001). These findings confirm other report that show that BMI increases with age in reports of
Saudis and others [36-46].
The frequencies of leanness, normal weight, overweight, obesity grade I and II and morbid obesity in the total study group was 2.9%, 18.7%, 27.0%, 24.4%, 16.4% and 10.5% respectively. We showed that 47.8% of non-pregnant women aged 20-39 years were overweight or obese (BMI ≥ 25kg/m2), 45.9% were obese (BMI ≥ 30kg/m2) and 17.7% were extremely obese (BMI ≥ 40kg/m2). Our prevalence estimates are higher than those from Ogden et al, who published a prevalence data from NHANES 1999-2004 [47]. In their analysis of 2003-2004 NHANES data specifically, 51.7% of non-pregnant women aged 20-39 years were overweight or obese (BMI ≥ 25kg/m2), 28.9% were obese (BMI ≥ 30kg/m2) and 8.0% were extremely obese (BMI ≥ 40kg/m2). We showed the frequency of obesity was higher compared to other reports which reported an obesity prevalence of 26.1% and 18.8% respectively and morbid obesity in 4.5% and 2.3% respectively 22,36. Two reports in 1994, one reported obesity in 41.9% and morbid obesity in 5.18% of females, while in the same year Khashoggi et al reported 64.3% of Saudi females to be obese [24,25]. However, due to the difference in the nature of the study group, it must be stressed that it is difficult to compare the results of the present study with those reported previously. Al Nuaim et al in two separate studies in 1997, reported 29.4% and 27% to be overweight, while El-Hazmi reported 25.2% of Saudi females aged between 14-70 y to be overweight [19-21]. Our data shows that as many as 2.9% of the Saudi females can be classified as lean which is lower than previously reported (10.17%) 36. According to the Health Survey for England 2011 data, morbid obesity rates are higher for women (3.2%) than for men (1.7%) 33. However, some data should be interpreted with caution as there is a margin of error due to the small proportions [48].
Clinical decision-making is driven in part by the prevalence of the condition in the general population. Obesity is considered to be a lifestyle disease, a result of modern living which has led to the creation of an obesogenic environment [49]. The need for effective weight management strategies is described in the mass media as well as in the healthcare literature [50]. In spite of public awareness of nutrition and fitness, of educational initiatives, and of the regulation of food marketing and other strategies, obesity continues to be a significant health risk for female Saudis. The impact of this health problem is described in terms of significant morbidity and mortality to childbearing-age women [51]. Childbearing-age women are a priority population for weight management initiatives because not only does maternal obesity affects the mother’s health, it is associated with delivery complications and complications with the child’s health, including a higher rate of birth defects [51].
The barriers, attitudes and motivators that affect weight management of childbearing age women are important to understand when considering measures to improve weight management of this high risk group [35,52,53]. These Saudi females present an ideal group for implementation of awareness programs as they can apply this information to prevent obesity development in themselves, their family members and their children.
This paper has provided evidence to the high frequency overweight and obesity amongst non- pregnant women of child bearing age resident in a sample size of our population exist. Results of our investigation must be interpreted in light of some limitations such as the cross-sectional design, which does not let to establish any causal relation with respect to obesity state and only provides mere associations. Considering the goal population, a larger cohort would have probably provided a greater power of the statistical analyses.
Conclusion
The frequency of overweight and obesity among women of childbearing age remains a critical public health
concern. Clearly, despite the small sample size, this study has posed important public health issues that
require immediate attention from the health authority. Unless immediate steps are taken to contain the
increasing prevalence of obesity, the health care costs for chronic diseases will pose an enormous financial
burden to the country.
Acknowledgments
We are grateful to the staffs of the endocrinology department at King Fahad Armed Forces Hospital for
their valuable contributions in data collection. The authors have no conflict of interest to disclose.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!