Biography
Interests
Yilima Chisha1, Biruk Wogayehu2* & Tamrat Toma3
1Department of Public Health, Arbaminch University, Arbaminch, Ethiopia
2Department of Pharmacy, Arbaminch College of Health Sciences, Arbaminch, Ethiopia
3Department of Medicine, Arba Minch University, Arbaminch, Ethiopia
*Correspondence to: Dr. Biruk Wogayehu, Department of Pharmacy, Arbaminch College of Health Sciences, Arbaminch, Ethiopia.
Copyright © 2019 Dr. Biruk Wogayehu , et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Hypertension is an overwhelming global challenge with high morbidity and mortality rate. Analysis
of the global burden of hypertension revealed that over 25% of the world’s adult population had
hypertension in 2000, and the proportion is expected to increase to 29% by 2025. The prevention
and control of high blood pressure has not received due attention in many developing countries.
Adherence to therapies is a primary determinant of treatment success. Poor adherence attenuates
optimum clinical benefits and therefore reduces the overall effectiveness of health systems.
To determine prevalence and associated factors of adherence to antihypertensive drugs among
hypertensive patients at Arbaminch general Hospital, Ethiopia, 2017 GC.
Institutional based cross-sectional study was conducted among 160 hypertensive patients in chronic
follow up clinic at Arbaminch general Hospital from September-December 2017 GC. A structured
questionnaire was used as data collection tool. Mo risky medication adherence scale was used for
labeling patients as adhered and non-adhered for antihypertensive drugs. Data cleaning, coding,
categorizing, merging and analysis carried out by STATA version 12. Descriptive statistics was
done and presented accordingly. Bivariate binary logistic regression analysis was done to select
potential candidates for the full model at P-value cutoff point ≤ 0.25 and multivariable binary
logistic regression analysis was made to estimate the independent effect of predictors on adherence.
Model diagnostic tests were done, final model fitness was checked using Hosmer and Lemeshow
chi square test. Finally, statistical significance was tested at P-value <0.05.
More than half (64.6%) of the study participants were found to be adherent to their treatment.
Distance from the hospital (AOR=3.786, 95%CI =1.77, 8.09) and co morbidity (AOR=5.664,
95%CI=1.93, 6.65) were found significantly associated factors with treatment adherence.
Only 64.6% of the study subjects were found to be adherent to their treatment. Factors such as
distance from the hospital and number of co morbidities were associated with adherence behavior
of patients. Early diagnosis and management of co morbidities, adherence counseling and patient
education about the disease and its treatment are important to improve adherence status of patient.
List of Abbreviations
AMGH: Arbaminch General Hospital
BP: Blood Pressure
HTN: Hypertension
ROC: Receiver Observed Characteristics
SNNPRS: Southern Nations nationality and People Regional State
WHO: World Health Organization
Introduction
Hypertension (HTN) or high blood pressure (systolic blood pressure ≥140mmHg and diastolic blood
pressure ≥90mmHg) is an overwhelming global challenge with high morbidity and mortality rate [1].
Analysis of the global burden of hypertension revealed that over 25% of the world’s adult Population had
hypertension in 2000, and the proportion is expected to increase to 29% by 2025. The prevention and control
of high blood pressure has not received due attention in many developing countries. Adherence to therapies
is a primary determinant of treatment success. Poor adherence attenuates Optimum clinical benefits and
therefore reduces the overall effectiveness of health systems [2-4].
Low adherence is a key factor in explaining impaired effectiveness and efficiency in the pharmacological treatment of hypertension. However, little is known about which factors determine low adherence in actual practice. Although there is shortage of extensive data, 10.5% of the Ethiopian population has been estimated to have HTN. Approximately 30% of adults in Addis Ababa have BP above 140/90mmHg or reported use of antihypertensive medications [4]. Poor adherence to antihypertensive medications is an obstacle in the management of hypertension resulting in high rate of hospitalization and death [5,6].
WHO report estimates that adherence to antihypertensive medications ranges from 52% to 74%. It also identified non adherence to medical treatment as a major public health concern, especially in patients with chronic conditions, e.g. hypertension. It is now evident from WHO data that coronary heart disease and cerebro vascular disease are increasing so rapidly that they will rank Number one and five respectively as causes of global burden by the year 2020 [7]. In Africa, 15% of the population has hypertension [8].
According to the WHO, more than 80% of deaths from hypertension and associated cardiovascular diseases now occur in low and middle-income countries and this is particularly common among people of low socioeconomic status [9].
Poor adherence is associated with bad outcome of the disease and wastage of healthcare resources [2,10]. Clearly, interventions to improve adherence with antihypertensive agents are needed, if such interventions are to be successfully designed, targeted, & cost effective, it is critical to understand the complex reasons for non-adherence and to identify those that are modifiable [1]. In Ethiopia, particularly in the study area, nothing is known about the adherence status and associated factors. Considering that HTN is a difficult disease for adherence to treatment due to the required change in lifestyle habits and active participation of the individual in antihypertensive medication therapy [11].
Generally, antihypertensive therapy should be maintained indefinitely [10]. However, findings in clinical practice have raised concerns about under treatment and non-adherence to antihypertensive treatment hampering the effectiveness of these medications [12].
Poor adherence has been attributed to unnecessary over-prescription of drugs, substantial worsening of diseases, avoidable increases in hospital admission rates, longer hospital stays, leading to a significant medical burden [13,14]. It also compromises the efforts of the health care system, policy makers and health care professionals in improving the health of populations. As a result, substantial numbers of patients do not get the maximum benefit of medical treatment resulting in poor health outcomes, lower quality of life increased health care costs and erodes public confidence in health systems.
Therefore, poor adherence to anti-hypertensive therapy is usually associated with bad outcome of the disease and wastage of limited health care resources in our setup. Therefore, the aim of this study is to assess the prevalence and factors contributing to medication adherence among adult patients with hypertension on follow up in Arbaminch general hospital (AMGH), Southern Ethiopia.
Methods
This cross sectional study was conducted at Arbaminch general hospital from April 2016 to October 2017
G.C. Arbaminch hospital was located at Arbaminch town, the capital city of Gamo Gofa zone, which is
505km form Addis Ababa (capital city of Ethiopia) and 280Km from Hawasa, center of southern nation’s
nationality and people regional state (SNNPRS). Arbaminch has two sub cities, Secha and Sikela. The
hospital is located at Secha which is the administrative center of Arbaminch town. Though Arbaminch
hospital is technically a regional hospital, it is acting as a referral hospital and provides preventive, curative
and rehabilitative care for 100,000-200,000 people per year and of them more than 400 patients were
hypertensive.
All cases of hypertension that were on follow up at AMGH who started taking antihypertensive drug
treatment at least for three months.
All cases of hypertensive patients who come during study period and who fulfill inclusion criteria.
Hypertensive patients of age18 years and above receiving antihypertensive treatment as outpatients at the
hypertensive illness follow-up care unit in AMGH during study period.
Those patients who were not capable of hearing and speaking and had known mental disorders or serious
illness.
Sample size determination formula for single population proportion was used, that is
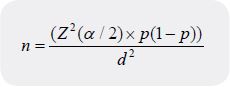
Where:
n- The required sample size
p- The proportion of the study subjects who were found to be adherent to their treatment in Gondar (64.6%).
z- A standard score corresponding to 95% confidence
d- The margin of error and is 5%
α= level of significance
Sample size will be:
ni = z2pq= (1.96)2(0.646)(0.354) = 351
d2 = (0.05)2.
Using the above formula, the initial sample size was 351, Which is less than 10,000 so that considering the finite population proportion (FPP) designed as “nf ”
Sample size determination formula for single population proportion was used, that is
nf = ni/1+ (ni/N) = 351/ (1+351/255) =146
Taking the non-response rate to be 10% the final sample size is 160.
Systematic random sampling method was used to select the respondents by every interval of two until the
total sample size fulfilled.
K value were calculated by
K=N/n = 400/160 ~= 3. Every other 3 patients were interviewed when they come for follow up at the chronic care clinic
A structured questionnaire was adopted from different study. The English version of the questionnaire was
adapted in such a way that it includes all the relevant variables to meet the objectives of the study and then
translated in to Amharic version. The Amharic version was again translated back to English to check for
consistency of meaning. The data was collected by BSc nurses who are working in the respective hospital.
A questionnaire was tested by 5% volunteer hypertensive patients before data collection. Investigators
were closely followed the data collection process at the spot. Data cleaning was performed to check for
completeness, consistency, extreme and missed values.
The data was entered to Microsoft excel software package and transferred to STATA version 12 for analysis.
Descriptive statistics was done and summarized using frequency, graph and percentage. Binary logistic
regression analysis was applied; Bivariate logistic regression analysis was done to select potential candidates
and explanatory variables with preset p-value ≤ 0.25 were included in the multivariable logistic regression
analysis to estimate the independent effect of predictors on adherence status. Step wise back ward elimination
model building procedure was done and model was compared by likely hood ratio test. Interaction and
cofounder were tested and cutoff point was beta change greater than 20%.
After fitting the final full model, multi collinearity was checked by variance inflation factor and cutoff point is mean VIF > 10 to have significant collinearity among predictors. The prediction performance of final fitted model was checked by receiver observed characteristics (ROC) curve and 70% will be acceptable discriminatory range. Overall model fitness was checked by Hosmer and Leme show chi-square test. Associations between adherence to anti-hypertensive drugs and predictors were summarized by using odds ratio and statistical significances were tested by Wald chi-square test at 95% CI.
Ethical approval was taken from Arbaminch University, College of Medicine and Health Science, School
of medicine. Permission to undertake the study in follow-up unit was obtained from the medical director’s
office of the hospital. Each study participant was adequately informed about the purpose, method, anticipated
benefit and risk of the study by the data collectors. Verbal consent was obtained from study participants and
anonymity was maintained to ensure confidentiality.
Results
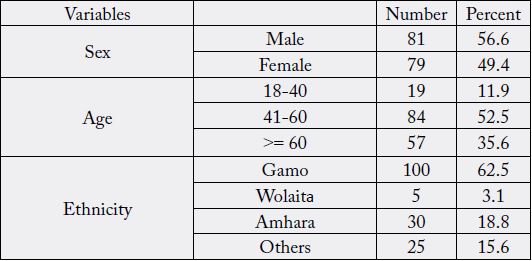
A total of 160 study participants were interviewed making the response rate 100%. As it is depicted below
table 1), males compromising 81(50.6%) of the population which is almost equal to female counter parts79
(49.4%). Regarding to age of the respondents, 84(52.5%) were in the age group between 41-60yrs.Whereas
35.6%, and11.9% of the respondents were in age group above 60 and 18-40years respectively. Out of 160
respondents, 62(38.8%) of the respondents have attended their education up to grade 7-12 and the 18.8%
were attended grade 1-6.
Majority of respondent in the study area 118(73.8%) earn a monthly income above 1000 Ethiopian birr and 29(18.1%) of the participants earn a monthly income between 501-1000 ETB and the rest 13 respondents have a monthly income below 500 birr. Regarding about employment status, 53(33.1%) of the respondents were merchants and 34(21.3%) were government employee. Whereas, students compromise 1% of the population, house wife women were found to account for 9.4% of the participants. Orthodox Christians and the Gamo ethnic group accounted for 84(52.5%) and100 (62.5%) of the respondents respectively.
Majority, 136 (85%) of the respondents were urban by resident. One hundred forty-one (88.1%) reported to be married and 3.1% are reported to be single. Pertaining to distance of respondents from hospital, 105 (65.6%) were live less than half an hour on single trip to reach to the hospital (Table 1).
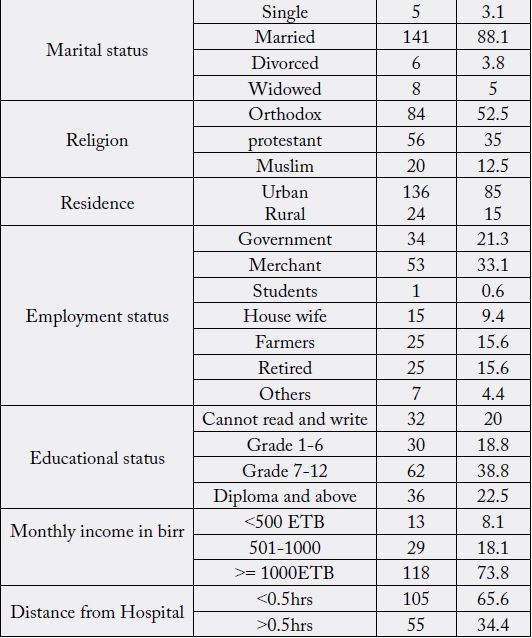
In the current study, among 160 participants, 112(70%) had controlled blood pressure. Regarding the
treatment, about 75(46.9%), were on treatment for 2-4 years, 92(57.5%) were on mono-therapy, 73(45.6%)
were took one pill per day and 20(12.5%) took three and above pills per day. More than two- third of the
participants, 116(72.5%), had no co-morbidity like diabetes, heart and kidney diseases. Out of 160 patients,
91(56.8%) take medicine once daily the remaining 15(9.4%) take medicine three times and above. Out of
the total 160 patients, 118(73.8%) had no fear of drug toxicity and the remaining 42(26.3) are feared of
drug toxicity.
Majority of the respondents, 147 (91.9%), were knowledgeable towards hypertension (HTN) and its treatment. Almost all, one hundred fifty-eight (98.8%) participants had good patient-provider relationship. Out of 160 patients majority 151(94.4%) are favorable attitude towards HTN and the remaining 9(5.6% ) are not favorable (Table 2).
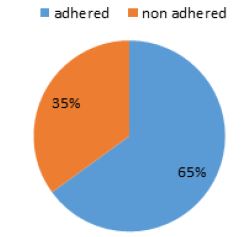
In this study, the overall prevalence of good drug adherence to antihypertensive medications was 65%.
(Figure 1)
The association of selected socio-demographic, clinical and other characteristics on adherence status was
investigated using both the bivariate and multivariable logistic regression technique. Accordingly, variables
considered in the bivariate analysis were: age, sex, residence, marital status, religion, educational status,
income, employment status, number of co-morbidities, BP level, distance, dosage frequency, duration of
treatment, number of medications, coverage of drug cost, knowledge about HTN and Patient provider
relationship. Explanatory variables with p value up to 0.25 were included in the multiple logistic regressions
(see on table 3).

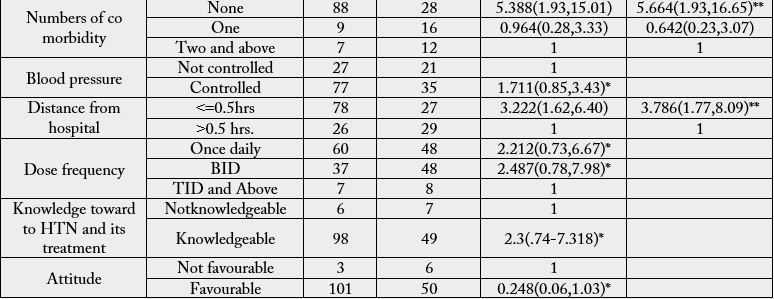
Note: - ** statistically significant * variables with p value of greater than 0.25 in crude analysis omitted from entering in to the model.
Finally distance which is less than 0.5 hr from the hospital and having no co-morbidity remained to be significantly associated with adherence to treatment of HTN. The multivariable logistic regression showed that as the distance from the hospital decreased, the adherence to treatment of HTN got improved. The odds of adherence to antihypertensive drugs is more than three times higher when we compare patients with distance from the hospital less than 0.5hr with their counter parts. (AOR = 3.78, 95% CI = 1.77, 8.09). The odds of adherence among study participants with no co-morbidities was 5.66 times higher than those who had two co-morbidities (adjusted OR= 5.66, 95%CI 1.96, 16.65) (Table 3).
Discussion
In many developing countries, maintaining good adherence to antihypertensive medications remained the
most important challenge. Adherence to antihypertensive medications contributes for controlled blood
pressure and the prevention of complications. Only 65% of the study subjects were found to be adherent
to their treatment. It is comparable with what has been reported from Gondar university referral hospital
(64.6%) [2]. the adherence to antihypertensive treatment found in the current study was also higher than
that of 57% found in the study done in Pakistan [15]. This difference is due to majority of respondents
having controlled BP in our study. Longer distance was a big barrier for adherence to treatment. Distance
from the hospital was found to be significantly and independently associated with the adherence status
of the respondents. Those patients from distant areas were less likely to be adherent as compared to study
subjects who are closer. This finding is supported by the study done in Gondar and India [2,14]. Patients
who take long to come to the clinic have certain characteristics that promote non-adherence, which also
delayed them from coming for review and possibly collecting drugs from the hospital when they refill the
antihypertensive.
The current study revealed that the numbers of co morbidities among HTN patients had significant associations on adherence behavior. This finding is supported by studies conducted in Gondar University Hospital [2], Addis Ababa Black lion hospital [16]. Co-morbidities can worsen the conditions of the patient and make them unable to adhere to their antihypertensive medications. Patients with no co morbidities were more likely to adhere to their treatment than those with two and above co morbidities. The possible reason could be if there is co -morbidity, they would have pill burden and if drugs are taken orally, they may cause gastrointestinal upset. All these might cause to miss antihypertensive medications. Additionally, when patients have additional health problem, their attention might be diverted towards the newly developed disease. Patients with more number of co morbidities could suffer from serious complications and complex treatment regimens which were favorable conditions not to adhere to their medications.
Limitation of the Study
This study has the following limitations: self-reporting was used as the only method of measuring adherence.
This method has the disadvantages of recall bias and eliciting only socially acceptable responses and hence,
may overestimate the level of adherence. In addition, it did not consider HTN patients who did not visit the
hospital during the time of the study. Hence, the extent of generalizability is limited only to those similar
patients who are on chronic illness follow up care. Since it is cross-sectional study, unable to detect causal
inference.
Conclusions
In conclusion, more than half of the study participants were found to be adherent to their treatment. Factors
such as distance from the hospital and number of co-morbidities were associated with adherence behavior
of patients. Early diagnosis and management of co morbidities, adherence counseling and patient education
about the disease and its treatment are important to improve adherence status of patients.
Recommendations
Administrative body of AMGH should increase health facility giving emphasis to health education towards hypertension.
To health professional, especially nurses should emphasis on the awareness creation related to hypertensive complications and the benefit of adherence behavior of the patients. Also to increase organized continuous health education concerning hypertension might be the increase for adherence among these patients.
To municipality of Arba Minch town to conduct mass health education and offering health education (information) for the public on hypertension and adherence of drugs increase the awareness of the community and attitude to comply with their medic.
Declarations Section
We declare that we do not have competing interests.
First of all, we would like to thank Arbaminch University College of health sciences for providing an ethical
approval and fund to conduct this study. Next, we would also like to give our heartfelt for officials and
professionals of Gamo Gofa zone health department and Arbaminch general Hospital for permission to
undertake the research and for welcomed face. Finally, we would like to gratitude data collectors, friends and
all individuals who helped directly or indirectly for the success of this study.
Y.C.D, is main author, conceived, designed and coordinated the study. M.S, T.T, S.S T.F and B.W participated
in formal analysis and interpretation of the data.
Y.C prepared original draft of the manuscript coordinated the data collection process, funding acquisition and supervision of data collectors.
T.F and S.S review and editing of the manuscript; all authors read and approved the final manuscript.
This study was funded by Arbaminch University
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!