Biography
Interests
Helmy, O.*, Mezouari, F. A., Tahiri, M., Rhaoussi, F. Z. E. L., Haddad, F., Hliwa, W., Bellabah, A. & Badre, W.
Hepatology and Gastroenterology Department, Ibn Rochd UHC, Casablanca, Morocco
*Correspondence to: Dr. Helmy, O., Hepatology and Gastroenterology Department, Ibn Rochd UHC, Hassan II University Casablanca, Morocco.
Copyright © 2022 Dr. Helmy, O. et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Abbreviations
HBV: hepatitis B virus
HCV: hepatitis C virus
SBP: Spontaneous Bacterial Peritonitis
HE: Hepatic encephalopathy
HCC: Hepatocellular carcinoma
HRS: hepatorenal syndrome
HCV RNA: Hepatitis C virus ribonucleic acid
NASH: Non alcoholic steato-hepatitis
NAFLD: Non alcoholic fatty liver disease
AALD: Alcoholic associated liver disease
Introduction
Liver disease, including cirrhosis, is an important cause of mortality in middle east and north Africa and
worldwide. It was the eighth leading cause of death in 2015 [1]. Various chronic liver diseases end by
liver cirrhosis [2,3]. The common complications of liver cirrhosis are ascites, jaundice, variceal bleeding,
spontaneous bacterial peritonitis (SBP), hepatic encephalopathy (HE), hepatocellular carcinoma (HCC) or
hepatorenal syndrome(HRS) [4]. This phase of the disease has been designated ‘‘decompensated cirrhosis’’
[5]. In Morocco, viral hepatitis is widely spread making it the leading cause of cirrhosis [6,7].
Despite the global growing economic and public burden of cirrhosis, data on the epidemiology of viral and non viral cirrhosis are extremely limited in Morocco.
The aim of this epidemiological study was to compare the baseline characteristics, recent trends in the first cause of hospital admissions and in-hospital mortality attributable to that cause between patients with viral and non viral related liver cirrhosis in a Moroccan cohort of 400 patients admitted to the hepatology and gastroenterology department of Ibn Rochd university hospital in Casablanca. Accordingly, clinical decisions can be made to improve the prognosis for Moroccan patients who are at higher risk for adverse outcomes.
Materials and Methods
A retrospective analysis was conducted using the medical record databases of Ibn rochd university hospital
in Casablanca, Morocco. Patients who had been hospitalized for the first cirrhosis-related complications
including ascites, variceal bleeding, SBP, HE, HRS, portal thrombosis, HCC or acute on chronic liver failure
were included. We determined the causes of admission and in-hospital death by reviewing the discharge
records. Medical records of 400 hospital admissions (400 patients) were reviewed. The study population
comprised 400 patients with decompensated HBV and HCV-related liver cirrhosis or non viral related
liver cirrhosis who had been hospitalized for the first time in Ibn Rochd hospital from November 2019 to
March 2022. HBV-related liver cirrhosis was recorded on the chart in case of hepatitis B surface antigen
had been present. HCV-related liver cirrhosis was documented on the chart in the presence of antibody to
HCV and HCV RNA in the serum. Patients with excessive alcohol consumption together with HBV or
HCV infection were classified as having liver cirrhosis with a combined cause. NAFLD (Non alcoholic fatty
liver disease) related cirrhosis was considered in patients who were obese and /or diabetic with the presence
of steatosis and absence of other causes. However, biopsy was not taken to confirm NASH (non alcoholic
steato-hepatitis) or AALD (alcoholic associated liver disease).
Data are expressed as means±standard deviation for continuous variables or as counts (percentages) for
categorical variables. The t-test was used to compare continuous variables, and the chi-square test was used
to compare categorical variables. A p-value of <0.05 was considered to indicate statistical significance.
Results
From November 2019 to March 2022, 400 patients were admitted (159 with viral related liver cirrhosis and
241 with non viral related liver cirrhosis). The mean age of patients with viral related cirrhosis patients and
non viral related cirrhosis was 61±9.4 and 56.2±15, respectively; p<0.0001. More male patients had viral
related liver cirrhosis while more females had non-viral related liver cirrhosis (table 1). HBV and HCV
related liver cirrhosis was the leading the cause of liver cirrhosis (159 patients 39.8%), among patients who
had been hospitalized due to cirrhosis complications, followed by non-alcoholic fatty liver disease (NAFLD)
(52 patients 13%), autoimmune hepatitis related cirrhosis (45 patients 11.3%) and alcoholic cirrhosis (30
patients 7.5%) (figure 1).

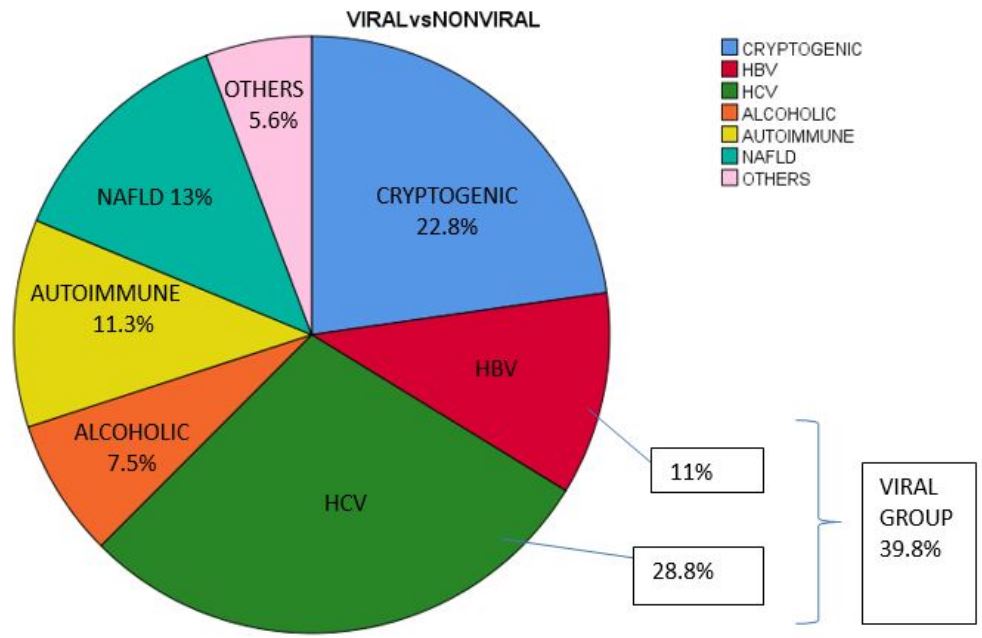
HCV, hepatitis C virus; HBV, hepatitis B virus.
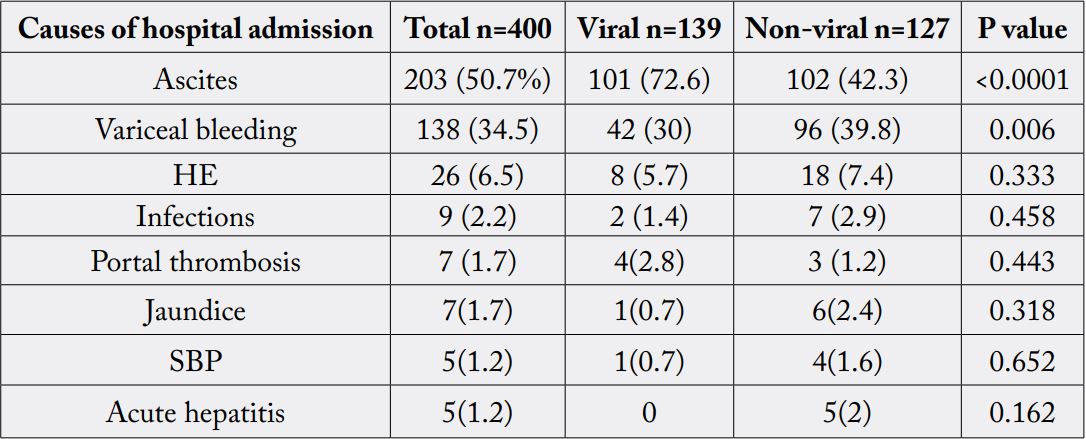
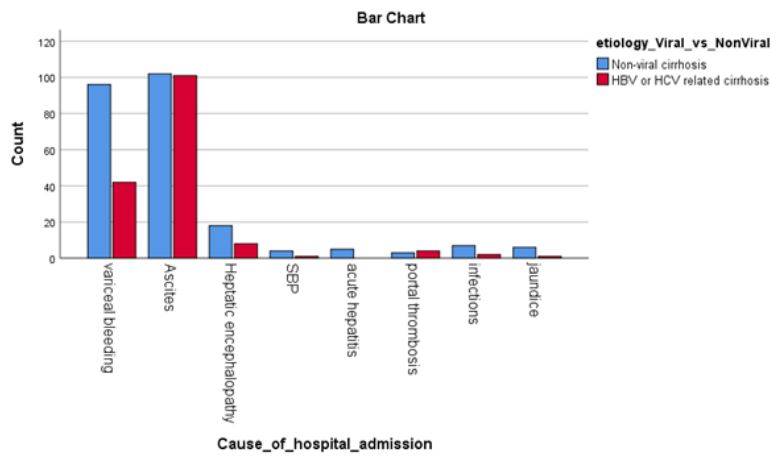
The most frequent causes of the first hospital admission in both groups were ascites (203 patients 50.7%)
and variceal bleeding (138 patients 34.5%) followed by HE (26 patients 6.5%). The proportion of infections
(ex. urinary infections) as a cause of first hospital admission was low at 2.3% (9 patients). The less frequent
causes were portal thrombosis, jaundice, SBP and acute hepatitis (table 2). The proportion of ascites, as a
first complication, in viral related cirrhosis was significantly higher than that in non viral cirrhosis (72.6%
vs 42.3%, p <0.0001). The study revealed that HCC was found in 14 patients who were admitted for other
causes such as ascites (11 patients 78.6%, p =0.034), variceal bleeding (1 patient 7% p=0.05) and HE (2 patients 14% p=0.229). Regarding child pugh score at first hospital admission, 122 patients (30.5%) were
score A, 181 patients (45.3%) were score B and 97 patients (24%) were score C.
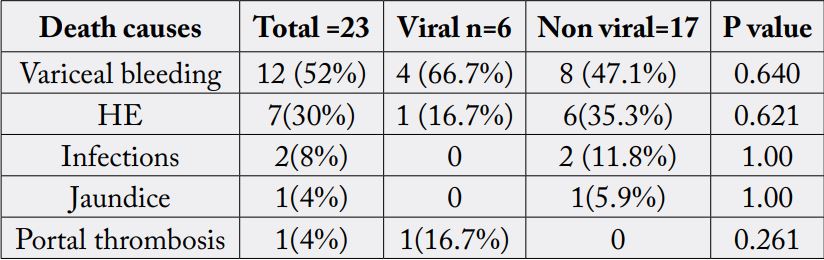
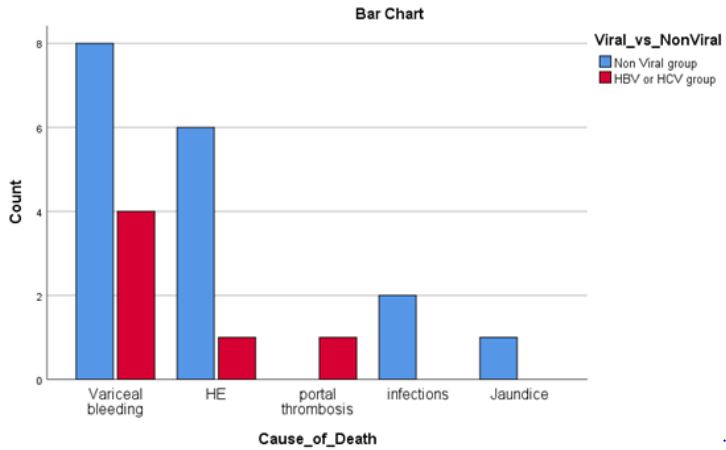
The in-hospital moratility rate at first hospital admission was 5.7% (23 patients). Variceal bleeding (12
patients 52%) and HE (7 patients 30%) were the most frequent causes of in-hospital deaths (table 3). While
the proportion of variceal bleeding in viral group (4 patients 66.7%) was higher than that in non viral group,
HE showed a higher proportion in non viral group (6 patients 35.3%). 19 patients (82%), who died at first
hospital admission, had advanced child pugh score (score B and C).
Discussion
Cirrhosis is one of the major causes of mortality, accounting for about 77,000 deaths per year in Middle East
and North Africa [1]. Despite the substantial burden of HCV and HBV related liver cirrhosis on public
health and the economy, few studies have investigated the epidemiology of viral and non viral related liver
cirrhosis in Morocco. This study retrospectively analyzes the epidemiology at the first hospital admission in
cirrhotic patients and the causes of in-hospital morality among viral and non-viral related liver cirrhosis in
the university hospital of Casablanca, Morocco. In this study, we found that the proportions of ascites and
variceal bleeding accounting for hospitalization were the highest in both groups. We also found that that
the major cause of in-hospital death was variceal bleeding in viral related liver cirrhosis, while in non-viral
related liver cirrhosis, variceal bleeding and HE showed the highest proportion.
In Morocco, the most common cause of liver cirrhosis is reportedly HCV followed by HBV [6] [7]. However, the prevalence of HCV and HBV-related liver cirrhosis is expected to decrease with the introduction of vaccination, potent antiviral agents and by launching the national campaign to eliminate HCV. The proportion of NAFL related cirrhosis is considerably high in Morocco because it is considered the first cause of cirrhosis in non-viral causes and the second cause of all causes according this study. This is probably due to the 6-fold global increase of the prevalence of obesity over the last 4 decades [8]. Additionally, there is an increase in diabetes in the world among adults [9]. Although there is limited data on the epidemiology of alcoholic liver cirrhosis, it seems that alcoholic associated liver disease is not a prominent cause of cirrhosis.
HCC was not a cause of first hospital admission in cirrhotic patients in this study but it was found in some patients admitted for other causes. The majority of cases who had HCC were admitted for ascites.
In-hospital mortality in cirrhotic patients with acute decompensation is high and it is higher than that of patients with other diseases [10]. The fact that there are numerous factors that determine hospital mortality must be taken into account and they include disease stage, complications, infections, organ dysfunction, acute-on-chronic liver failure, and clinical status upon admission [11-13]. In our patient cohort, in-hospital mortality at first admission was 5.7% and the most frequent causes of death were variceal bleeding and HE. The majority had high child-pugh scores. These percentages are considered high and this may be due to shortage of some important medications such as somatostatin which is fundamental in variceal bleeding. Another cause is that transferring cirrhotic patients to ICU takes time due to shortage of beds especially during the epidemic of the COVID-19 and due to the bad prognosis of cirrhotics with high child-pugh scores giving them less priority. These data suggest the need for new public health measures for the prevention and early and opportune diagnosis of this disease, such as increasing the awareness of screening and treatment of hepatitis C virus, so that the development of complications that darken the outcome in patients with cirrhosis can be prevented and delayed.
This study has some limitations. First, we did not perform a liver biopsy to confirm the alcoholic cirrhosis and NASH related cirrhosis. Due to the absence of definitive diagnostic criteria for the pathologic diagnosis of alcoholic cirrhosis and NASH, we used clinical diagnosis of alcoholic cirrhosis and NAFLD in addition to radiological findings in NAFLD. Secondly, the enrolled patients did not present the entire population of hospitalized patients with cirrhosis in Morocco.
Nevertheless, the strengths of this study were that a relatively large number of patients were enrolled in the analysis. Additionally, we investigated the trend of complications and in-hospital deaths among cirrhotic patients who were hospitalized in a university hospital stratified according to viral and non-viral cirrhosis.
Conclusion
In conclusion, the proportions of ascites and variceal bleeding were the highest among causes of first admission in both viral and non-viral related cirrhotic patients. Variceal bleeding was the major cause of in-hospital death in both groups and HE was the second major cause in non-viral group. The adaptation of public
health measures directed towards prevention and early and opportune diagnosis of this disease is necessary
to prevent the development of complications and improve outcome in cirrhotic patients.
Conflict of Interests
No conflicts of interest are to be declared.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!