Biography
Interests
Mamah Cyril Chukwukama1, Maduka-Okafor Ferdinand, C.1, Onwubiko Stella Ngozi1, Okoloagu Nkiruka Mary2*, Ugwu Kenneth, O.3, Anyalebechi Okey Charles1, Ebede Samuel, O.4 & Umeh Rich, E.1
1Department of Ophthalmology, University of Nigeria Teaching Hospital, Ituku-Ozalla PMB 01129 Enugu, Nigeria
2Department of Ophthalmology, Enugu State University of Science and Technology Teaching Hospital, Parklane
Enugu, Nigeria
3Department of Microbiology, University of Nigeria Nsukka Enugu Nigeria
4Department of Medical Microbiology, University of Nigeria Teaching Hospital, Ituku-Ozalla PMB 01129
Enugu, Nigeria
*Correspondence to: Dr. Okoloagu Nkiruka Mary, Department of Ophthalmology, Enugu State University of Science and Technology Teaching Hospital, Parklane Enugu, Nigeria.
Copyright © 2021 Dr. Okoloagu Nkiruka Mary, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
To determine the risk factors for conjunctival bacteria flora in pre-operative cataract patients.
This was a descriptive, cross-sectional, hospital-based, prospective study involving 104 consecutive, consented patients scheduled for cataract surgery at University of Nigeria Teaching Hospital
Enugu in 2017. Patients using any form of antibiotics, with previous intraocular surgery or ocular
inflammation were excluded from the study. The participants’ socio-demographic profile, medical
and social histories were obtained through interviewer-administered questionnaire. Conjunctival
swab was obtained from the inferior fornix of the eye scheduled for surgery. Data was analysed
using Statistical Package for Social Science version 23. Logistic regression analysis was done to
identify the factors. The level of significance was at p<0.05.
The participants were mainly females 67(64.4%), with a mean age of 64±2SD years. The conjunctival
swab bacteria isolation rate was 36.5%. Advanced age, male gender, illiteracy, residency in rural
areas and tobacco use were associated with increased bacterial isolation but only age was statistically
significant, p=0.02. Use of topical medications (anti-glaucoma and artificial tear) significantly
reduced bacteria growth, p=0.03. However, in the multiple regression models, only age remained
statistically significant.
Strict precautionary measures should be directed to illiterate male patients on tobacco use residing
in rural areas especially, the elderly ones, to avert the menace of post-operative endophthalmitis.
Introduction
Worldwide, cataract surgery is a highly cost-effective treatment for the leading cause of avoidable blindness,
usually with good visual outcome, barring devastating complications by endophthalmitis. Studies have shown
that greater proportion of post-operative endophthalmitis are caused by the contamination of microorganism
from the conjunctiva and eyelid during surgical manipulation and peri-operative period [1-4].
Endophthalmitis is a severe and dreaded complication of cataract surgery. It could cause permanent loss of vision as well as the eye ball, if not identified and managed appropriately. The collateral damage caused by this devastating complication could be a source of discouragement and barrier to uptake of cataract surgery.
Several factors such as advanced age [5-9], male gender [5,10], climatic and geographical locations [11,12], use of topical medications [8,13,14], and immunosuppressive conditions [8,15,16] have been documented to influence conjunctival bacteria. Understanding the epidemiological characteristics of conjunctival bacteria flora is important to avert the menace of post-operative endophthalmitis. It offers the Ophthalmologist a high index of suspicion and informed decision on early detection of disease and intervention to restore vision.
No previous study has been done in south-east Nigeria. Hence the decision to conduct this study in UNTH, a major hospital in the region aimed at generating data for an evidence-based policy and protocol on the management of patients scheduled for cataract surgery.
Methods
University of Nigeria Teaching Hospital (UNTH) Ituku-Ozalla, Enugu was established in 1960. It is located
along Enugu-Port Harcourt expressway, 15 Kilometers from Enugu Metropolis, the capital of old eastern
Nigeria. Enugu State is one of the 36 States of the Federal Republic of Nigeria. It is located in the South-
Eastern geo-political region of Nigeria. It falls within the transitional forest- savannah region with a mean
annual rainfall of 1,200-2,000mm, and has two main seasons: rainy and dry seasons. UNTH provides health
care and functions as a referral centre for the entire Southeast, South-south, North-central and occasionally
other parts of Nigeria. The Ophthalmology department runs daily weekday clinics, theatres and 24 hours
emergency services. It maintains eye centre in one of the outposts of the teaching hospital where residents
are sent for rural posting. The department runs regular outreach program where eye care is provided and
patients requiring further management referred to the centre. Cataract cases are brought to the hospital
complex for surgery. Every category of patients are seen and treated. The Medical Microbiology department
is within the hospital complex and is about five minutes walking distance apart from Ophthalmology clinic
and ward. It has excellent synergy with Ophthalmology department.
This was a descriptive, cross- sectional, hospital-based, prospective study involving 104 consecutive patients
scheduled for cataract surgery from June to September 2017 at UNTH that meet the eligibility criteria, and
voluntarily consented to participation.
Consenting patients (consent from patients’ caregiver for children) booked for cataract surgery, irrespective
of age.
Patients who were on topical or systemic antibiotics or had used same within two weeks of presentation,
history of contact lens wear, previous intraocular surgery or active ocular inflammation. Patients who did not
give consent and those due to age or other peculiarities were not cooperative.
Minimal sample size (N) was determined using formula below for calculating cross sectional study sample
size
Z1-a/2 at 95% confidence index is 1.96
p: is estimate positive result from previous research. A positive result of 41.9% was recorded in a research done in south-west, Nigeria [12].
d: is the precision (allowable error) which will be 10%

= 93.519 ≈≈ 94 eyes.
Attrition of 10% will give 9.4 eyes.
N ≈≈ 104 eyes.
All consecutive consenting patients irrespective of age scheduled for cataract operation were recruited into
the study until the estimated sample size was obtained. Only the eye scheduled for the operation was
included even in patients with bilateral operable cataract.
Existing and new patients seen, diagnosed and booked for cataract surgery were evaluated for eligibility and
recruited into the study. After obtaining consent, the structured and pre-tested questionnaire comprising of
three sections: - socio-demographic, clinical and laboratory sections was administered by the researchers.
Having explained the procedure to each participant, a pair of sterile surgical gloves was worn by the
principal researcher; the lower lid manually retracted by gentle downward pull to expose the inferior
conjunctival fornix. Participants were requested to gaze up to avoid irritating or injuring the cornea, then,
conjunctival swab was obtained from the inferior conjunctiva fornix by swabbing from the lateral end to the
medial end using a sterile swab stick without touching the eye lashes or lid skin. Each swab stick specimen
was taken within 30 minutes to Medical Microbiology and Parasitology Laboratory, unit for immediate
inoculation.
In the laboratory, following standard method, swab was promptly inoculated onto three culture media:- blood
agar, nutrient agar and MacConkey agar aimed at optimal isolation and was incubated at 37°C overnight
according to the CLSI standard guidelines [17].
The statistical package used to analyze the data collected was IBM SPSS version 23. Chi-square tests were
used to identify the factors associated with the conjunctival bacteria growth in the univariate analysis. The
level of significance considered was P < 0.05. Multiple logistic regression analysis was carried out to confirm
the significant associations established using Chi-Square tests.
Results
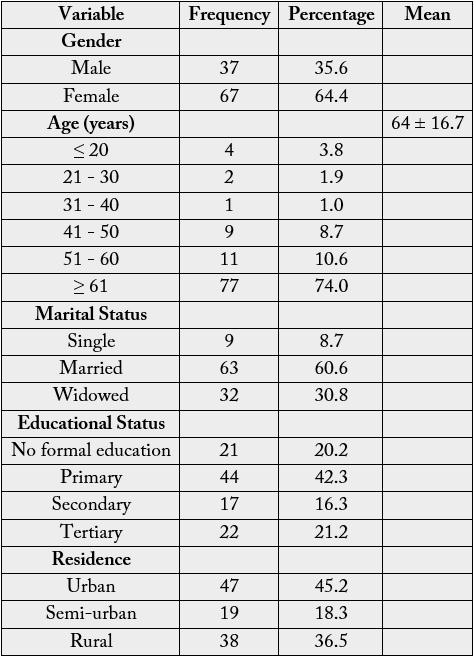
The participants comprised of 37 (35.6%) males and 67 (64.4%) females with a mean age of 64±2SD years.
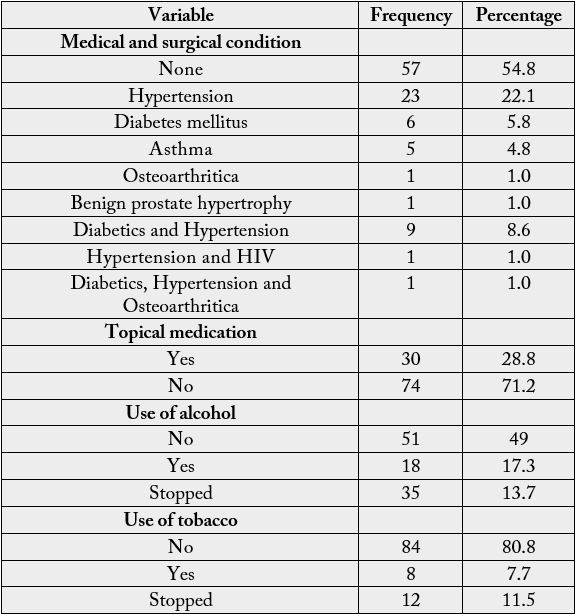
Other characteristics were as shown in tables 1 and 2.
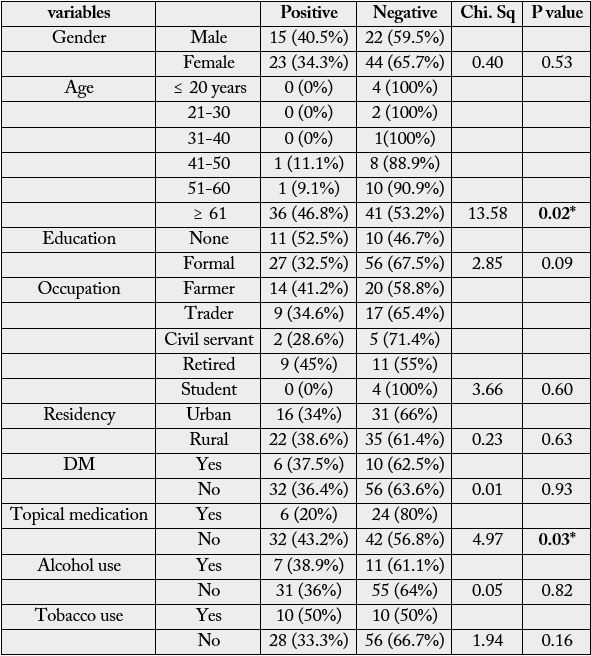
Thirty-eight participants had conjunctival bacteria growth. The conjunctival swab bacteria isolation rate was 36.5%.
In the univariate analysis, age p=0.02 and use of topic medications p=0.03 (anti-glaucoma and artificial tear) significantly increased and reduced conjunctival bacteria growth respectively, table 3.
But when they were subjected to the multiple logistic regression analysis, only age remained statistically significant, table 4.

Discussion
The participants comprised of more females than males with a mean age of 64±2SD years. This demographic
profile is similar to findings in other studies [18,19]. This is not surprising because cataract is known to be
age-related, increasing with advancing age [1].
In this study, age significantly increased conjunctival bacteria growth. This finding has been documented elsewhere in several studies [5-9,13,18]. It is believed that the visual challenges cataract imposes on patients could negatively affect their personal hygiene, coupled with decreasing immunity associated with normal aging process. Strict precautionary measures should therefore be directed to the elderly patients, in order to avert the complications of post-operative endophthalmitis.
Use of topical medications (anti-glaucoma and artificial tear) significantly reduced conjunctival bacteria growth, in this study. Similar report was made in other studies [8,13,14]. The wash out effect of the topical medications and the antiseptic properties of benzalkonium, the preservative in most topical medications may explain this finding.
The male gender has been associated with increased conjunctival bacteria growth [5,10,18,19]. However, similar observation was made in this study, though not statistically significant. In contrast, other studies [8,20] did not find any association with gender. The observed gender differences in adherence to use of medications [21] and conjunctival bacterial flora [22] may possibly explain this report.
Elsewhere, diabetes mellitus [8,16], alcohol [23] and tobacco [24] use have been associated with increased bacterial isolation. In the present study, these factors were weakly associated with increased conjunctival bacteria growth. The immunosuppressive effect of these factors may account for this finding. More robust studies with large sample size of populations with these factors to investigate this association is therefore advised.
Illiteracy and residency in rural areas were also found to be weakly associated with increased conjunctival bacteria growth in this study. Therefore, it is suggested that future studies should be designed to explore the influence of these socio-economic factors on conjunctival bacterial growth.
The hospital-based nature of the study may limit generalisation of the results to the larger population.
Beside that, the bacterial isolates were characterized based on their colonial morphology, Gram reaction and
biochemical activities. Molecular techniques were not deployed in the characterization of the isolates. Also
molecular techniques were not used to specifically identify the DNA sequence with mutations responsible
for the observed resistance.
Conclusion
Advanced age has remained the single most important risk factor for conjunctival bacterial growth in
patients scheduled for cataract surgery in the study area. However, strict precautionary measures should be
directed to illiterate male patients on alcohol and tobacco use residing in rural areas especially, the elderly
ones, to avert the menace of post-operative endophthalmitis.
Key Messages
• Understanding the epidemiological characteristics of conjunctival bacteria flora is important to avert the
menace of post-operative endophthalmitis.
• Advanced age, male gender, illiteracy, residency in rural areas and tobacco use were associated with increased
bacterial isolation.
• Use of topical medications (anti-glaucoma and artificial tear) significantly reduced bacteria growth.
Declarations / Compliance with Ethical Standards
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!