Biography
Interests
Ana Lazarova* & Antonio Gligorievski
University Clinic for Surgery Disease St.Naum Ohridski Skopje, R. Macedonia
*Correspondence to: Dr. Ana Lazarova, University Clinic for Surgery Disease St.Naum Ohridski Skopje, R. Macedonia.
Copyright © 2021 Dr. Ana Lazarova, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Intestinal obstruction is a condition in which intestine is obstructed because of any mechanical
or non-mechanical reasons. It accounts for 20% of all surgical admissions for acute abdomen.
Computed tomography (CT) is currently the exam of choice for bowel obstruction because has
higher specificity in reporting the etiology, site and grade of obstruction, and the presence of bowel
ischemia, affecting the surgical decision.
To determine the sensitivity and specificity of contrast-enchased CT for diagnosing the small and
large bowel obstruction.
This is prospective study which includes 100 patients diagnosed with bowel obstruction in the
period from January 2016 to July 2020 in the University Clinic for Surgery Disease St. Naum Ohridski Skopje. All of the patients were with clinic presentation of acute abdomen. Primary
conventional X- ray on abdomen was done and bowel distention with developed air-fluid levels was
found. This was an indication for CT so the reason for bowel obstruction to be found as well as the
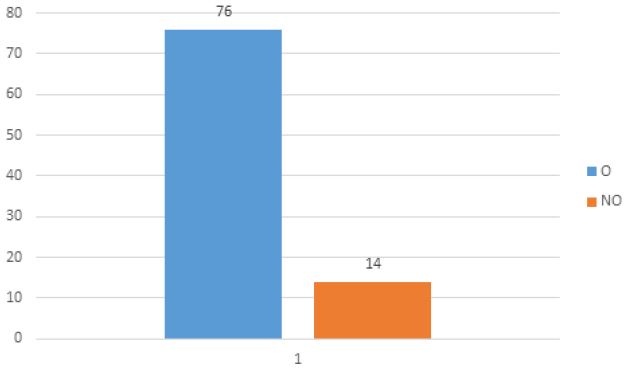
level, site and grade of obstruction.76 from 100 patients underwent operative treatment whereas
14 patients were treated conservatively and with nasogastric tube decompression. The results of
surgical treatment in resolving intestinal obstruction and the finding for etiology were taken as the
gold standard in evaluating the accuracy of CT in detecting the causes of intestinal obstruction.
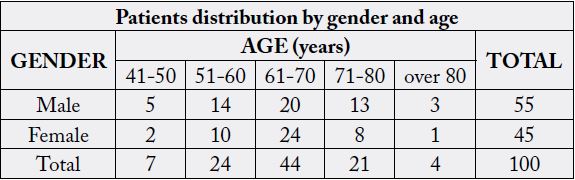
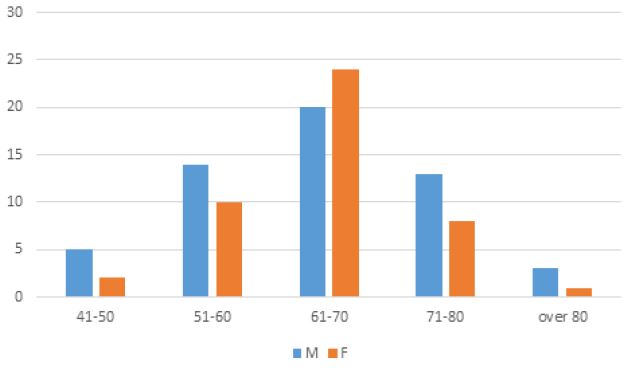
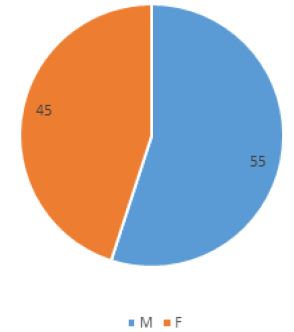
This study included a 100 patients aged from 44 to 81 years.55 from the patients were male and
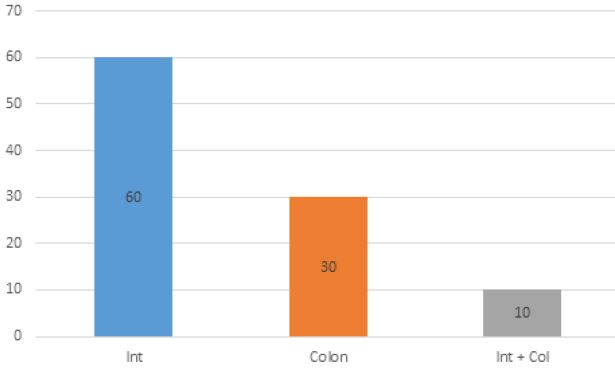
45 female .60 from the patients had small bowel obstruction and 30 patents had large bowel
obstruction, whereas in 10 patients there was bowel obstruction on the small and large intestine
in the same time. In 39 patients small bowel obstruction was caused by adhesive bends and in
that case CT scan made prediction for that reason made on exclusion. In two cases ileus was as a
result of pseudomembranous colitis, one as small bowel obstruction and one was small and large
bowel obstruction. There were 3 patients with acute diverticulitis on sigmoid part of the colon. In
one case it was small bowel obstruction and in two patients there were small and secondary large
bowel obstruction. One case was presented with peritoneal carcinomatosis as a reason for bowel
obstruction. Seven from the patients with bowel obstruction were with intestinal ischemia as a
result of mesenteric thrombosis. Five of them were only with small bowel obstruction a two were
with small primary and then developed large bowel obstruction.11 patients presented with bowel
obstruction as a result of herniation. In two patients complications from Morbus Chron were the
reason for small bowel obstruction. There were 30 patients present with large bowel obstruction.
The main cause of it in 24 patients was neoinfiltrative process in the wall of the bowel. In 6 patients
the reason for large bowel obstruction was sigmoid volvulus. CT is more sensitive than radiographs
and its ability to demonstrate the cause of bowel obstruction is around 80% of the cases.
This study is a clear indication of the importance of contrasts enhanced CT in the evaluation of
intestinal obstruction. High accuracy in detecting the etiology of intestinal obstruction makes it the
most important diagnostic method for adequate resolution of intestinal obstruction.
Introduction
Intestinal obstruction is a condition in which intestine is obstructed because of any mechanical or nonmechanical
reasons. It accounts for 20% of all surgical admissions for acute abdomen. To understand the
bowel obstruction which has high rate of “surgical abdomens” is important to have an inside look in the
major causes for it. Radiology is important in confirming the diagnosis and identifying the underlying cause
[1,2].
Computed tomography (CT) is currently the exam of choice for bowel obstruction because has higher specificity in reporting the etiology, site and grade of obstruction, and the presence of bowel ischemia, affecting the surgical decision [3].
The causes of bowel obstruction are variable and often require urgent management. Delay in diagnosis and management can result in bowel ischemia and death [4].
Diagnostic approaches include history, physical examination and radiological investigations in combination. Routinely X-ray abdomen in addition to history and physical examination is done for diagnosis of intestinal obstruction. Its diagnostic accuracy is about 40-80% [5].
Bowel obstructions are usually divided according to where the obstruction occurs, and since imaging appearances, underlying pathology, and treatment differ, these are discussed separately. Small bowel obstruction only includes small intestine and there is competent ileocecal valve so there is no distention of the large intestine [6].
Small bowel obstruction (SBO) accounts for 80% of all mechanical intestinal obstruction, the remaining 20% results from a large bowel obstruction. It has a mortality rate of ~5% [7].
Small-bowel obstruction (SBO) is caused by a variety of pathologic processes. Causes can be divided into congenital and acquired. Acquired causes may be extrinsic causing compression, intrinsic, or luminal [8].
Although large number of SBO patients is treated successfully with nasogastric tube decompression, the mortality of SBO increases to 25% if bowel ischemia is present with delayed surgical management. A challenge in the clinical management is that clinical presentation, physical examination findings, and laboratory tests are insufficient to make an accurate diagnosis of SBO, but the management has changed considerably since then due to advancements in imaging technology, such as computed tomography (CT) [9,10].
The most common cause of SBO in developed countries is intra-abdominal adhesions, accounting for approximately 65% to 75% of cases, followed by hernias, Crohn disease, malignancy, and volvulus. In contrast, SBO in developing countries is primary caused by hernias (30-40%), adhesions (about 30%), and tuberculosis (about 10%), along with malignancy, Crohn disease, volvulus, and parasitic infections. The general trend in developing countries is an increased incidence of SBO from adhesions, with a higher incidence of laparotomies [11-13].
As a rare cause of SBO is endometriosis, the endometrial implants are typically on anti- mesenteric edge of the bowel. And also masses are cause of small bowel obstruction and it may be: extrinsic neoplasm, intraabdominal abscess, aneurysm and hematoma with their outside pressure on the bowel wall might lead to obstruction [14].
In intrinsic bowel wall causes are important different inflammatory process for example Morbus Chron, Tuberculosis, eosinophilic gastroenteritis, to be mentioned [15].
Tumors are a rare case when small bowel obstruction comes in matter because only less than 2% of all gastrointestinal (GIT) tumors belong to the small intestinal tumor. Here are included: GIST, adenocarcinoma and lymphoma. But more common is small bowel involvement of metastatic disease, as for a peritoneal carcinomatosis with an extrinsic serosal disease [16].
Other reason is radiation enteritis which produces adhesive and fibrotic changes in the mesentery with luminal narrowing and dysmotility. Important thing is that it may cause an obstruction is in the late phase after more than a year after therapy [7].
Intestinal ischemia is also one of the often causes of small bowel obstruction as a result of occlusion or stenosis of the mesenteric artery or vascular supply there is a small bowel wall thickening and obstruction [17].
Luminal narrowing that lead to bowel obstruction might be as a result of intraluminal hematoma by trauma, iatrogenic, anticoagulant therapy, Henoch- Schonlein purpura [2].
Intussusception as a case of small bowel obstruction is rare in adults less than 5 % but it can be a lead point that may relate to neoplasm, adhesion or foreign body. In this case leading mass should be carefully interpreted and differentiated from the soft -tissue pseudotumor that represents the intussusception itself [18].
The classic presentation is with abdominal pain, distension, and failure of passage of flatus and stool. As dilatation of the colon increases, the risk of perforation also increases. Perforation may occur at the site of obstruction, or more proximally secondary to ischemic change, which may be implied by the presence of intramural gas or decreased mural enhancement. Signs of peritonism, sepsis, and shock may develop when perforation occurs [20].
The underlying etiology of large bowel obstructions is age-dependent, but in adulthood, the most common cause is colonic cancer (50-60%), typically in the sigmoid. The second most common cause in adults is acute diverticulitis (involving the sigmoid colon). Together, obstructing tumors and acute diverticulitis account for 90% of all causes of large bowel obstruction. While adhesions are the leading cause of small bowel obstruction, for practical purposes, they do not tend to cause large bowel obstruction [21].
Overall causes of large bowel obstruction include: malignancy, most common is colorectal carcinoma which accounts 50-60%, also pelvic tumors as direct spread of metastatic disease. Another reason are colonic diverticulitis, volvulus (cecal volvulus with 1-3% and sigmoid volvulus with 3-8%), ischemic colitis [22].
Material and Methods
This is prospective study which includes 100 patients primary diagnosed with bowel obstruction in the
period from January 2016 to July 2020 in the University Clinic for Surgery Disease St. Naum Ohridski
Skopje.
All of the patients were with clinic presentation of acute abdomen sent from the Department of Urgent medicine to the Department of Radiology for further investigation. Primary conventional X- ray on abdomen was done in all patients and bowel distention with developed air-fluid levels was found. This was an indication for contrast - enhanced computer tomography (CT) scan to be done so the reason for bowel obstruction to be found as well as the level, site and grade of obstruction. Most of the patients 76 from 100 underwent operative treatment whereas 14 patients were treated conservatively and with nasogastric tube decompression.
The results of surgical treatment in resolving intestinal obstruction and the finding for etiology were taken as the gold standard in evaluating the accuracy of CT in detecting the causes of intestinal obstruction.
Results
This study included a 100 patients aged from 44 to 81 years old with an average aged of, 55 from the patients
were male and 45 female (Table 1, graphic 1, graphic 2)
60 from the patients had small bowel obstruction and 30 patents had large bowel obstruction, whereas in 10 patients there was bowel obstruction on the small and large intestine in the same time (Graphic 3).
76 from 100 patients underwent operative treatment whereas 14 patients were treated conservatively and with nasogastric tube decompression (Graphic 4)
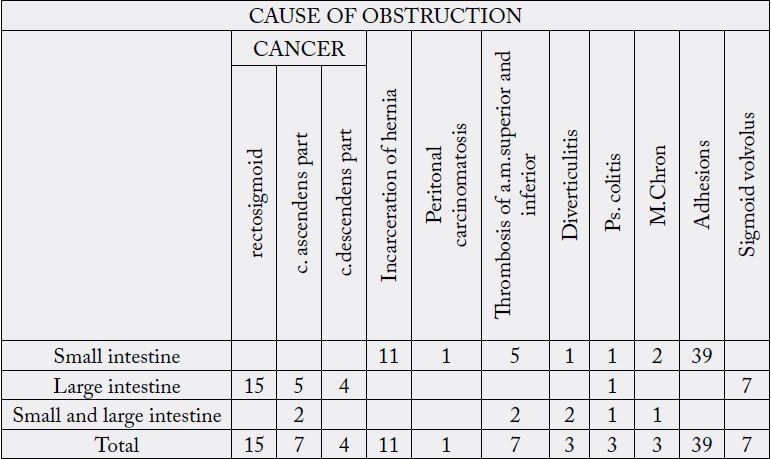
In 39 patients small bowel obstruction was caused by adhesive bends and in that case CT scan made prediction for that reason made on exclusion. In two cases ileus was as a result of pseudomembranous colitis, one as small bowel obstruction and one was small and large bowel obstruction. There were 3 patients with acute diverticulitis on sigmoid part of the colon. In one case it was small bowel obstruction and in two patients there were small and secondary large bowel obstruction. One case was presented with peritoneal carcinomatosis as a reason for bowel obstruction. Seven from the patients with bowel obstruction were with intestinal ischemia as a result of mesenteric thrombosis. Five of them were only with small bowel obstruction a two were with small primary and then developed large bowel obstruction.11 patients presented with bowel obstruction as a result of herniation. In two patients complications from Morbus Chron were the reason for small bowel obstruction. There were 30 patients present with large bowel obstruction. The main cause of it in 24 patients was neoinfiltrative process in the wall of the bowel. In 6 patients the reason for large bowel obstruction was sigmoid volvulus (Table 2).
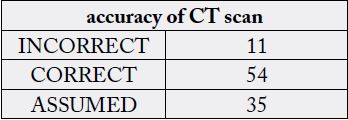
In 54 patients diagnose for the level and the reason of bowel obstruction was correct interpreted with CT scan, as it was verificated operatively. In 11 patients there was incorrect made diagnose with CT scan, whereas in 35 patients the diagnoses for obstruction was made on prediction because small bowel obstruction was caused by adhesive bends and in that case CT scan made prediction for that reason made on exclusion. Those 35 patients were taken as a correct interpretation for calculating the ACCUARACY of CT scan to demonstrate the cause and the level of bowel obstruction which in this study is 79% (Table 3).
Discussion
In this study we present the importance and ability of CT scans for detecting the type of bowel obstruction,
the level of it together with the cause, etiology of bowel obstruction. All patients under clinic presentation
of acute abdomen from the Department of Urgent medicine were sent to the Department of Radiology for
X- ray of the abdomen.
In all patients sings of ileus with developed air-fluid levels and dilated loops were found. In this study CT scan was the only tool for diagnose the cause of ileus. CT is more sensitive than radiographs and its ability to demonstrate the cause of bowel obstruction is around 79% of the cases. There is a variety depending whether it is small or large bowel obstruction.
There is a consensus regarding the use of CT in the evaluation of patients with SBO, and many studies reported that CT is a helpful tool to diagnose SBO, identify causes and the transition point, and most importantly, detect ischemia, which requires prompt surgical intervention [23,24]. However, CT findings about such points exhibit variable diagnostic performance. For example, the sensitivity of CT for diagnosis of SBO varied from 50% to 100%, and the specificity values varied from 57% to 100% [25-27].
Diagnosis of adhesive bands witch are the commonest case of small bowel obstruction is made of exclusion as that is because adhesive bands are not seen on CT [28,29].
In our study there were 39 patients with small bowel obstruction caused by adhesive bends and in most of the cases (35 from 39) CT scan made prediction for that reason made on exclusion.
In two cases ileus was as a result of pseudomembranous colitis, one only as small bowel obstruction and one was small and large bowel obstruction. CT suggested that the obstruction of the lumen was caused by the swelling of the wall of the intestine. Colonoscopy leads to the detection of pseudo-membrane. There were no signs of toxic megacolon, nor perforation so operative treatment was not needed, ileus resolve conservatively.
In this study there were 3 patients with acute diverticulitis on sigmoid part of the colon. In one case it was small bowel obstruction and in two patients there were small and secondary large bowel obstruction. Inflammation extends in to small bowel mesentery. In those patient’s bowel obstruction resolved conservatively. Because diverticulitis is known to be caused of small bowel obstruction a more conservatively approach was intended and initially surgery was avoiding, careful analyses of the sigmoid part of the colon and a local change in the colonic wall were enough for establishing the correct diagnosis. The small bowel loops become trapped in the inflammatory process resulting in fixation and narrowing.
One case was presented with peritoneal carcinomatosis as a reason for small bowel obstruction. There are not guidelines for surgical management of malignant bowel obstruction (MBO) caused by peritoneal carcinomatosis (PC), mainly when it involves elderly; so its treatment is still debated but in our case surgical palliation provided relief of obstructive symptoms.
Seven from the patients with bowel obstruction were with intestinal ischemia as a result of mesenteric thrombosis. Five of them were only with small bowel obstruction a two were with small primary and then developed large bowel obstruction. Mesenteric thrombosis can decrease the supply of blood to the tissues and cells of the bowel that lead to ischemia. It causes intestinal damage or the death of intestinal tissue, infarction. In all seven patients surgery was the option of treatment because the dead portion of the intestine must be surgically removed.
Incarceration of the hernia may be a cause of bowel obstruction, in this study 11 patients presented with small bowel obstruction as a result of herniation. Common types of hernias that cause intestinal obstructions include inguinal hernias, femoral hernias, and incisional hernias. CT scan as a method of diagnosis of incarcerated hernias was in all 11 patients presenting the adequate diagnosis confirmed after the surgery treatment.
In two patients complications from Morbus Chron were the reason for small bowel obstruction because when it comes to small bowel obstruction in Chron disease this one may related to acute flare with luminal narrowing secondary to transmural inflammation or cicatricle stenosis in long - standing disease and also due to adhesions or incisional hernias from previous surgery [27].
CT is currently the most widely used modality for assessment especially of large bowel obstruction and is not only able to confirm the diagnosis and localize the location of obstruction but in most instances also is able to identify the cause. The large bowel will be distended with a thinned stretched wall but should enhance (unless ischemic). If the ileocecal valve is competent then the small bowel may be mostly collapsed. It should be traced distally until a transition is found. The cause is often present at this point, although sometimes the obstructing lesion is distal to the apparent transition point [30,31].
In this study there were 30 patients present with large bowel obstruction. The main cause of it in 24 patients was neoinfiltrative process in the wall of the bowel, resulting to complete narrowing and obstruction. The carcinoma was visible in contrast enhanced CT scan. The commonest localization of the carcinoma was at rectosigmoid/sigmoid part of the bowel in 15 patients. In 5 was at colon ascendant and in 4 at colon descendent.
Bowel obstruction (BO) is a complication that commonly affects patients with colorectal cancer (CRC), and 25-40% of CRC patients suffer from this condition. In most of the cases bowel obstruction is the first presenting symptom/sign for exiting the malignant bowel disease [32].
In 6 patients the reason for large bowel obstruction was sigmoid volvulus.
Sigmoid volvulus (SV), the most common type of colonic volvolus, is a frequent cause of bowel obstruction. In the United States, CV is the third most common cause of large-bowel obstruction and is responsible for approximately 5% of all cases of intestinal obstruction and 10% to 15% of all cases of large-bowel obstruction. The sigmoid colon is the most common site of large-bowel torsion (80%), followed by the cecum (15%), transverse colon (3%), and splenic flexure (2%). Prompt diagnosis and treatment are critical in order to avoid the development of bowel ischemia [33].
Ten patients present with both small and large intestinal obstruction as a result of incompetent cecal valve, so primary small bowel obstruction affect the large bowel and vice versa. The cause of bowel obstruction in those 10 patients were: 2 patients acute diverticulitis, 2 patients colon ascendant cancer, 2 patients had mesenteric thrombosis resulting with intestinal ischemia, 2 patient with adhesive bends, and one with pseudomembranous colitis and with one Morbus Chron [34].
Conclusion
This study is a clear indication of the importance of contrasts enhanced CT in the evaluation of intestinal
obstruction. High accuracy, wich in this study is 79%, in detecting the etiology of intestinal obstruction makes
it the most important diagnostic method for adequate resolution of intestinal obstruction. The possibility
of visualization of the intestinal wall and evaluation of the possible occurrence of intestinal ischemia gives
importance in the planning of the treatment as well as the time for the surgical intervention.
All these possibilities of CT, detection of the type of intestinal obstruction, etiology as well as the level and severity of the condition are sufficient indicators that CT can be a gold standard in the diagnosis of intestinal obstruction.
Accuracy in properly diagnosing the cause of intestinal obstruction gives a radiological certainty that is necessary for the surgeon in further planning of treatment. This is especially important in large bowel obstruction, but although the sensitivity and specificity of CT in small bowel obstruction are less, they are not of lesser importance.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!