Biography
Interests
Ahmad Jebur1, Tammam Harfouch2 & Rim Harfouch1*
1Department of Biochemistry and Microbiology, Faculty of Pharmacy, Al Andalus University for Medical Sciences, Tartous, Syria
2Department of Cardiovascular Surgery, Cardiovascular Diseases Institute, Iasi, Romania
*Correspondence to: Dr. Rim Harfouch, Department of Biochemistry and Microbiology, Faculty of Pharmacy, Al Andalus University for Medical Sciences, Tartous, Syria.
Copyright © 2021 Rim Harfouch, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
The whole world is facing the COVID-19 pandemic caused by (SARS-CoV-2) virus, which was first reported in December 2019 in Wuhan, China, which was classified by the World Health Organization (WHO) as a public health emergency of international concern On January 30, 2020. Because of the exponential increase in the number of cases and deaths, many countries have adopted pandemic preparedness measures and proactive approaches, such as entry restrictions from affected countries; temperature screening; quarantine of those who have contacted with infected people, or those deemed to be in the incubation period; and public education.
Lack of resources is a problem in reporting COVID-19 cases in the majority of Arab countries, especially in Yemen, Libya, Sudan, and Syria. Civil wars have weakened infrastructure and divided governments, making it difficult to detect the virus and care for those infected. In this review, we summarize the status of COVID-19 disease in all Arab countries and the estimated number of cases and deaths by their governments.
Introduction
The whole world is facing the COVID-19 pandemic caused by (SARS-CoV-2) virus, which was first
reported in December 2019 in Wuhan, China. On January 30, 2020, the World Health Organization
(WHO) declared the COVID-19 a public health emergency of international concern [1].
Common symptoms of COVID-19 include acute respiratory illness (cold-like disease), hyperthermia (fever>38ºC), coughing, sore throat, and shortness of breath. Also, numerous sufferers may also experience digestive symptoms such as anorexia, diarrhea, and vomiting [2].
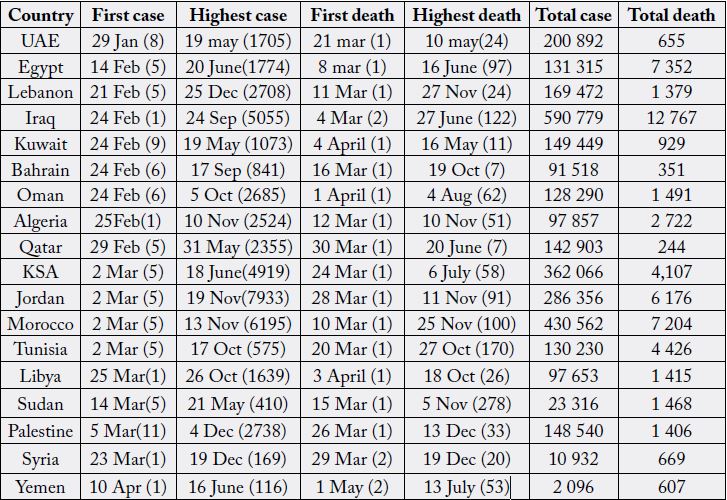
In the Arab world, the data show very low rates compared to those in Europe and in the United States. As of December 29th, there were (3,194,046) positive cases and (54,990) deaths. The highest numbers of new cases in the region were recorded in Iraq (590,790), then Saudi Arabia (362,066), and in third place Morocco (430,562) [3,4].
The following actions have been taken by the majority of Arab world countries: Effective contact tracing and quarantine action, in addition to systematic testing of suspected cases. Because of the exponential increase in the number of cases and deaths, many countries have adopted pandemic preparedness measures and proactive approaches, such as entry restrictions from affected countries; temperature screening; quarantine of those who have contacted infected, or those deemed to be in the incubation period; and public education and awareness. Lack of resources is a problem in reporting COVID-19 cases in the majority of Arab countries, especially in Yemen, Libya, Sudan, and Syria. Civil wars have weakened infrastructure and divided governments, making it difficult to detect the virus and care for those infected [4].
Some countries don’t have big difficulties (Morocco, Egypt, Gulf Countries, Saudi Arabia), but others are experiencing chronic problems aggravated by the COVID-19 situation (Sudan, Lebanon, Palestine, Yemen). If the duration of the pandemic increases, the situation risks becoming disastrous in most of these countries. In Syria, there are more than 6 million displaced people living in overcrowded refugee camps, which gives the virus a big opportunity to flourish, with tightly packed communities that lack appropriate health and sanitation services. It is true that the problem is particularly acute in the case of refugees and in the conflict in other zones. (Lebanon, Yemen, Iraq, Libya). The treatment protocols across countries are similar. They are using Hydroxychloroquine, Chloroquine phosphate, Remedesivir, and Lopinavir/Ritonavir, despite the inconclusive results on Hydroxychloroquine, several countries in the region including Morocco and Algeria continued to use this drug [5].
On 29th January 2020, the United Arab Emirates reported its first laboratory-confirmed cases. Then, after 3
months (19 May), the UAE recorded the highest rate of cases (1705 cases). There was a gradual improvement
in morbidity and mortality between June and September, as the lowest number of infections was observed
on August 4, After that, the rates gradually increased due to the new wave of Coronavirus, as on May 19, a
high rate of infection was observed. The cure rates are generally good, as the highest cure rate was observed
on September 6, 2020, with (2434) new cures, on 1ST January 2021 the total number of infections in the
UAE was 207,822 cases, 669 deaths, and 195520 recovered [6].
Egypt was the second Arab country to announce a corona infection on 14 February, reported its first
confirmed COVID-19 case (5 cases), a contact of a confirmed case with history of travel to China. On June
20, Egypt reported the highest cases of Corona (1774) cases, Days before it on June 16, the highest death
was recorded, 97 deaths, From the beginning of August for a period of 4 months, stable and low rates of
infection were recorded, reaching 89 cases on August 23, Then due to the new wave the rates were raised
again, on the first day of 2021. On 1st January 2021, there were 138,062 confirmed cases of COVID-19 with
7,631 deaths and 112826 total recoveries [7].
On 21st February 2020, Lebanon reported its first confirmed case who had traveled back from Qom, Iran.
One day later, Lebanon shut down public transport and banned flights to countries that had experienced
exponential growth patterns of COVID-19, including Iran, Italy, China and South Korea. By mid-March,
when the number of infections reached 99, the government issued stay-at-home orders, closed the borders,
and closed non-essential services [8]. Within 5 months, infection rates were stable and controlled, reaching
on 8th August to 5,951 cases, 70 deaths, and 2042 recoveries. Increasing trend due to mass testing of
repatriates late June, re-opening of port starting 2 July; community transmission started with multiple
clusters across the country The rates increased dramatically until it reached about 183,880 confirmed cases
on 1/1/2021, 1466 deaths and 107,521 cures due to the new wave of Coronavirus [9].
Iraq reported its first confirmed case who had traveled back from Qom On 24th February 2020. Iraq has been
in a stable period in the first 3 months due to the quarantine, During this period, 58,354 cases, 2,368 deaths,
and 3,107 recoveries were recorded on 4th July. After that, the incidence increased incrementally, reaching
on 24 September to 5,055 cases in one day and 122 deaths on 27th June 2020, gradually decreasing again 4
months later. Iraq is considered one of the countries with the highest record of Corona cases, with about
596,193 cases, 12,824 deaths and 541,746 recovered on January 2nd, 2021 [10].
Kuwait reported its first confirmed case on 24th February a citizen coming from Iran. The government
responded to this crisis with early public health interventions such as school and airport closures, curfews,
and restrictions on public gatherings. Despite these crucial measures, the disease continued to spread, with
the expatriate labour community particularly affected. Initially, the numbers were low and stable, with the
limits of dozens of cases per day until the beginning of April, when cases increased to reach their highest
levels on May 19, with 1,073 cases and on 16 May about 11 deaths, the gradual decline began in November.
On December 27th, the Ministry of Health began the COVID-19 vaccination campaign with priority groups of workers in the health sector, and no unexpected side effects were detected after about 48 hours had passed since the sample slice that received the COVID-19 vaccine during the opening Campaign demo. The last recorded statistics on January 2, 2021 were 150,869 cases, 936 deaths and 146,990 recovered [11].
On 24th February, Oman reported its first confirmed case who came from Iran. Analysis of the First showed
that 1304 Cases, 95.9% of cases were mild, 3.6% moderate, and 0.5% severe with a case fatality rate of 0.5%.
This trend is similar to many countries, interesting observation is the low mortality rate compared to western
countries and the high incidence of mild COVID-19, there is a chance that there might be a high incidence
of asymptomatic COVID-19 cases in Oman, Underdiagnoses is a possible problem in epidemiology studies
of COVID-19 since many cases are mild or asymptomatic.
By the end of 2020, a significant increase was observed in the rates, to reach 128,867 cases, 1499 deaths and 122,266 recoveries on January 2nd, 202. The Omani Ministry of Health started the vaccination campaign for the BioNTech-Pfizer vaccine, and the coverage rate for the country reached 28.8% on January 3rd [12].
On 24th February, Bahrain reported its first confirmed case who had travelled to the Islamic Republic of
Iran. The prevalence of COVID-19 disease in Bahrain was approximately 0.1%, with 2464 documented
cases on 25th April. A total of 114,110 tests had been conducted, reaching about 71 tests per 1000 people. Of
the 2464 cases, eight deaths had been recorded, 1189 cases had recovered and 1447 cases had been admitted.
All COVID-19 cases had been admitted to either an isolated COVID-19 ICU, hospital or isolation facility,
depending on the patients’ medical requirements. Later, within 6 months, the number of cases increased, as
the rate increased on September 17th to the highest rate, with 814 new cases and 3 deaths per day.
On December 16th, the Ministry of Health announced the start of the national vaccination process against Coronavirus, (Pfizer and Synotec). on January 3rd, 2021, the total numbers of individual vaccinated is 60,689, the number of total infections was 93,478, deaths 352, and the cure was 90,686 [13].
On 29th February, reported its first confirmed cases had travelled Iran. Qatar is one of the countries that have
the highest numbers of COVID-19. By July 11th, 103 128 infections had been laboratory-confirmed at a
rate of 36 729 per million population. The epidemic intensity in Qatar reflected the unique demographic and
residential dwelling structure of this country. As of July 5th, case severity rate was 3.4% and case fatality rate
was 1.4 per 1,000 persons. Attack rate (ever infection) was estimated at 53.5% on July 12th.
Qatar has experienced a large SARS-CoV-2 epidemic that is rapidly declining. The Qatar Ministry of Health announced the start of the vaccination process for the Pfizer Sputnik vaccine against Corona on December 23, The total number of cases reached 144,437 and 245 deaths and 141925 were cured on January 4th, 2021 [14].
The Kingdom of Saudi Arabia, confirmed the first COVID-19 positive case on March 2nd, 2020. For
the first time in the eight decades of the Muslim pilgrimage to the holy sites in the Kingdom of Saudi
Arabia (KSA). on 27th February 2020, KSA placed restrictions on inbound Umrah pilgrimage, placed a
ban on inbound travel of persons coming from COVID-19 affected countries and restrictions on travel of
Gulf Cooperation Council (GCC) citizens who have travelled to COVID-19-affected countries. Till 24th
August, 306,370 confirmed cases and 3619 died have been recorded, and a case-fatality rate of 0.6%, most
of which were in the main cities including Mecca, Riyadh, Jeddah, and medina. In mid-December, Saudi
Arabia began the vaccination program against Coronavirus, on January 4th, the total number of infections
was 363,155, and 6,256 deaths and 354,609 recovered [15].
Since the first case, reported on 25th February 2020, in the department of Ouargla (southern Algeria),
before 5 days of the true beginning of a new outbreak in the department of Blida on 1st March 2020, which
became the epicenter of the epidemic.
The epidemic curve has shown multiple features, three peaks in the epidemic curve, at the end of April and in mid-July and mid -November. The number of reported cases showed an increase until late April/early May. A decrease was then observed, which pushed the national authorities to start relaxing the implemented measures and containment, that was subsequently associated with an increase in the number of cases. It has currently recorded 100,159 cases, making it one of the most affected countries in Africa along with South Africa, Egypt, Nigeria, Morocco and Ghana, with 2769 deaths and 67,808 recovered [16].
On March 2nd, 2020, the first case of COVID-19 infection was reported in Casablanca city, which was imported
from Italy by a Moroccan individual, many travelers from Europe have tested positive for COVID-19 in
different cities such as Casablanca, Marrakesh and Fez. Since seven imported cases have emerged, Moroccan
government decided to suspend flights to neighboring countries affected by COVID-19 such as Italy, Spain,
Algeria and France. Later, a first confirmed local case appeared on March 14th. Cases began to increase after
5 months from the onset of the disease reaching its highest peak on 16 November with 6,195 cases per day.
Later, the cases rate decreased to reach 443,146 cases 7,485 deaths and 413,393 recovered on January 3rd,
2021 [17].
The first confirmed case in Tunisia was reported on March 2nd, 2020. This led to the implementation of highlevel
preventive strategies, including physical distancing measures by the Tunisian government. From May
10th to July 13th, Tunisia recorded the lowest number of cases and deaths. On June 15th 2020, the Tunisian
government announced that it had taken control of Coronavirus but on 17th October, the highest number
5752 cases were reported in one day. Tunisia trends show an increase in cases since the country reopened its borders at the end of June. On January 2nd 2021, the total number of cases reached 143,544 cases, 4,800
deaths, and 107,049 recoveries [18].
The first confirmed case was reported on March 3rd. According to the World Health Organization Situation
Report 83 released on April 12th 2020, Jordan was classified with a “cluster of cases” transmission for the
virus. As of March 17th 2020, the government called for social distancing, seized all forms of inbound and
outbound movement or international travel, and enacted the Defense Law that transferred the authority to
the Minister of Defense to work and formulate orders according to the situation. Until September 1st, the
total number was 1716 cases, after that the rates increased suddenly until it reached the highest rate 7,933
cases on 17th October. Later, it decreased to reach 298,208 cases, 3,903 deaths, and 278,929 cures on January
4th 2021 [19].
The first case was detected on March 5th 2020. Later, 152 deaths were reported on August 27th 2020 with
more than 26,764 total number of infected cases. The phase of COVID-19 epidemics can be decomposed as
an exponential growth. The Palestinian Ministries of Health in both Gaza and Ramallah have acknowledged
that their capacity to contain the spread of COVID-19 is limited by ongoing and pre-existing shortages
in health-care equipment, public health measures have erred on the side of caution and largely contributed
to a very low infection rate during the first 3 months of the crisis. Gaza has recommended that individuals
returning from outside Gaza through the Rafah or Erez crossing remain in quarantine for 21 days, instead
of 14 days. After August, the cases increased dramatically, reaching the highest rate on December 4th, with
about 2738 new cases, 33 deaths on December 13th. The latest statistics on January 3rd showed a decrease in
the infection rate, so that the total number of 159,043 cases was 1,609 deaths and 139,215 recovered [20,21].
On 14th March 2020, The first case and death in Sudan was reported. Since then, the numbers of cases
increased rapidly to reach the first peak in the epidemic curve on May 21st, with 410 new cases per day,
regardless of measures that were initiated by the federal and state government to combat the outbreak.
The COVID-19 cases in Sudan are low, but the mortality is higher (278 deaths in one day 5th December) compared with the total African cases. Outbreak rates decreased on September and rose again at a second peak in December due to the new wave of Coronavirus. The prevalence is high among males (60%) and people aged 15-29.9 years. Because Sudan has a small percentage of the population over the age of 65.8, which explains the high rate of infection among the youth (The majority of cases lived in the Khartoum State). On 4th January 2021 the total number was 23,316 confirmed cases and 1468 death [22].
On March 22nd 2020, the Syrian Ministry of Health confirmed the first case of COVID-19, Since then,
universities and public institutions in government-controlled areas have been closed and curfews imposed from 18:00 to 06:00 every day. COVID-19 infection rates and deaths in Syria are currently low, with just
over 177 cases and six deaths reported in early June 2020. In areas outside of government control, one case
was reported in the northeast of the country, while No cases have been reported in the northwest, Conflictaffected
countries like Syria face many challenges with health systems that have already been destroyed;
as such, SARS-CoV-2 can spread rapidly among the affected population, particularly among the most
vulnerable groups.
On October 1st 2020, Syria reopened Damascus Airport to international flights after it was closed for more than six months in light of strict measures to avoid the Corona virus, after which the largest number of reported cases was recorded since the beginning of the outbreak, most of them coming from Kuwait, Saudi Arabia, Lebanon and Jordan. On January 5th, Syria recorded 11,890 cases, 741 deaths, and 5,686 recoveries [23,24].
On 24th March 2020 the first confirmed case of coronavirus was recorded of a man in his seventies, by the
National Centre for Disease Control (NCDC) of Libya.
The first death was recorded officially on 3rd April 2020, of an 85-year-old woman who died in Tripoli. Libya is not well equipped to manage and control any pandemic due to the chaos and loss of central control since 2011, 17 of the 97 hospitals are closed, and most hospitals are operating at low performance. Only 40% of hospital inpatient beds are properly functioning, another major concern in Libya is the limited knowledge and public awareness of COVID-19 along with the socio-cultural norms of the gathering, which can facilitate its transmission.
As of May 12th 2020, there were 64 cases. The lower number of reported cases is due to fewer performed tests in Libya, with an average daily capacity of less than 50 tests. After June, the largest number of new cases and deaths recorded (the highest peak was recorded on October 26 with 1639 new cases and 26 deaths on October 18) associated with an increase in testing capacity from 3 laboratories initially to 15 functional laboratories. On 5th January the total number of cases was 102,456 cases, 1,536 deaths and 76,244 recovered [25].
On April 10th 2020, the first confirmed case of the COVID-19 pandemic was announced in Hadramout.
On April 29th, Aden recorded five new cases of COVID-19. at the same time, In Sana’a, although there
is insufficient data, it is believed that a few cases of COVID-19 were detected. It is not well known if
COVID-19 has particularly spread to Yemen from other neighboring countries such as Saudi Arabia and
other countries at the border, at the same time, Yemeni passengers were travelling from many different
countries to Yemen. Real data on the COVID-19 situation in Yemen is largely scarce. As of May 2020,
the World Health Organization provided Yemeni laboratories with 6700 RT-PCR tests only, which were
distributed to five laboratories across the country. On June 16th, the largest number of cases in Yemen
was recorded in one day, 116 new cases. The COVID-19 pandemic is another blow to a war-torn country, devastated by a 5-year blockade, and has not yet recovered from the deadly cholera and diphtheria epidemic
that began in 2016.
It is likely that COVID-19 spread in Yemen through Yemeni business workers or merchants who were traveling to China, Wuhan, before the lockdown. This is why it is believed that COVID-19 was spreading in Yemen earlier than announced, after that the rates decreased. The number of cases of COVID-19 in Yemen is expected to be more than what has been announced due to many factors including war conflicts that have destroyed the health infrastructure, on 5th January the total number of cases was 2,105 cases, 611 deaths [26].
Conclusion
Whilst COVID-19 epidemic trajectories for many Arab countries are similar, some countries do have
flatter curve than others due to prompt implementation of restrictive measures at the very initial stage of
a COVID-19 outbreak along with mass testing programs. Estimating the real impact of the coronavirus
pandemic on war-torn counties could prove to be challenging.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!