Biography
Interests
Premkumar Daivasikamani1*, Suresh2, Khoo Wei Chin1, Khoo Chun Yik1, Ang Shang En1 & Kodeesh Kanna Mona Kanna1
1Faculty of Medicine, AIMST University, Semiling, Kedah, Malaysia
2Consultant Gastroenterologist, Al Hilal Hospital, Muharraq, Bahrain
*Correspondence to: Dr. Premkumar Daivasikamani, Faculty of Medicine, AIMST University, Semiling, Kedah, Malaysia.
Copyright © 2021 Dr. Premkumar Daivasikamani, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Common cause of gastritis is due to the infection of Helicobacter Pylori infection producing the inflammation of the gastric mucosa. The other risk factors are medication, stress, radiation, bile reflux, consumption of spicy or starchy food, sedentary life and drinking alcohol and irregular meals. Gastritis is believed to be present in 30% to 50% of the population. Gastritis is diagnosed clinically and if complications arise by endoscopy. If patient complaints of dyspepsia endoscopy must be done to rule out gastric carcinoma. Gastritis is common in females and in the age between 21 to 23years. More common in Chinese students and doing medicine course. Sometimes there may not be a particular cause for them to develop gastritis.
Introduction
Gastritis is classified and diagnosed histologically as the inflammatory changes in the stomach mucosa.
Most important etiology of gastritis are Helicobacter pylori infection, irregular meals, nonsteroidal antiinflammatory
drugs (NSAIDs), stress, radiation, bile reflux, ischemia and eating spicy or starchy food,
sedentary life, and drinking alcohol. Though gastritis may be present in 30% to 50% of the population, most
of them are asymptomatic. Patients with gastritis normally presented with nonspecific clinical signs and
symptoms including epigastric pain, abdominal tenderness, bloating, anorexia, nausea, and with or without
vomiting. Gastritis symptoms may be aggravated by eating. Gastritis is can be present in 30% to 50% of the
population. Gastritis is diagnosed clinically and if complications arise by endoscopy. If patient complaints of
dyspepsia endoscopy must be done to rule out gastric carcinoma. Gastritis is common in females and in the
ages between 21to -23years. More common in Chinese students and doing medicine course. For them there
is no particular cause to develop gastritis.
Objectives
To identify the level of awareness and incidence of gastritis among the university students.
There is no association between awareness and knowledge of eating habits in prevalence of gastritis.
There is association between awareness and knowledge of eating habits in prevalence of gastritis.
Materials and Methods
A cross sectional study is used to assess the awareness and knowledge on association of eating habits to
prevalence of gastritis among AIMST University students. Independent variable in this study is the socio
demographic factors which include the gender, ethnicity, level of education, and family history of gastritis.
Dependent variable is the awareness and knowledge of eating habits in association with gastritis. In this
study, the students have selected their own university, AIMST University in Kedah, Malaysia to conduct the
study due to adequate availability of participants and feasible to conduct the study. Population of study are
AIMST University students from MBBS, Dentistry, Pharmacy, Biotechnology, Allied Health Professions
and Foundation Studies courses, in the age group of 18-26 year. Sample comprises of 400 AIMST University
students in the age group of 17-25 years. Inclusion criteria are the students from AIMST University with all
categories of age and gender. Exclusion criteria are AIMST students who had been diagnosed as gastritis by
Doctor. The data from sample is collected by a structured questionnaire about awareness is developed based
on the information drawn from the books and journals regarding assessing the awareness of gastritis. The
questionnaire is divided into three parts: questions on socio-demographics factors, attitude, and knowledge
regarding awareness of eating habits in association with gastritis. By using SPSS version 22 (trial version)
the data obtained was analyzed. The demographic data are described with the descriptive statistics. The chi-square test are carried out to find out associations among demographic data and the awareness and
knowledge of eating habits in association with gastritis.
Results
Pie Chart 1 Shows Frequency of Gender of the Subjects that have gastritis (N=81).
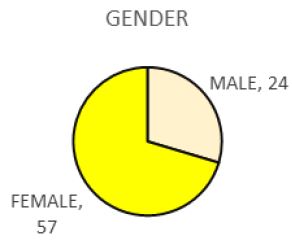
There are 24 males and 57 females out of 81 samples who had been diagnosed as gastritis by Doctor. Prevalence of gastritis among female is higher.
Pie Chart 2 Shows Frequency of Different Age Group of the Subjects that have gastritis (N=81).
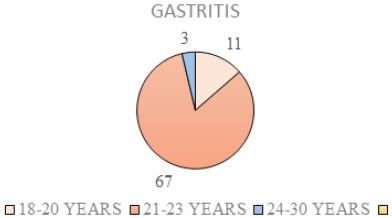
Out of 81 samples who had been diagnosed as gastritis by Doctor, there are 11 samples in the age group of 18-20 years, 67 samples in the age group of 21-23 years and 3 samples in the age group of 24-26 years. Prevalence of gastritis among age group 21-23 years is higher.
Pie Chart 3 Shows Frequency of Different Races of the Subjects that have gastritis (N=81).
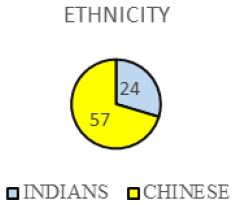
There are 1 Malay, 24 Indians and 57 Chinese among 81 samples who had been diagnosed as gastritis by Doctor. Prevalence of gastritis among Chinese is higher.
Pie Chart 4 Shows Frequency of the Subjects in Different Course of Study that have gastritis (N=81).
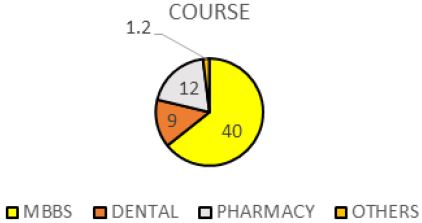
Out of 81 samples who had been diagnosed as gastritis by Doctor, there are 40 MBBS students, 9 Dentistry students, 12 Pharmacy students and 20 students from other course such as Biotechnology, Allied Health Professions and Foundation Studies. Prevalence of gastritis among MBBS students is higher. There are 62.50% MBBS students, 14.00% Dentistry students, 10.00% Pharmacy students and 13.50% students from other course such as Biotechnology, Allied Health Professions and Foundation Studies.
Pie Chart 5 Shows Frequency of the Subjects in Different Year of Study that have gastritis (N=81).
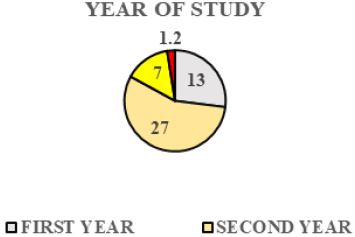
There are 13 Year 1 students, 27 Year 2 students, 7 Year 3 students, 33 Year 4 students and 1 Year 5 students among 81 samples who had been diagnosed as gastritis by Doctor. Prevalence of gastritis among Year 4 students is higher.There are 74.25% hosteller and 25.75% non-hosteller.
Pie Chart 6 Shows Frequency of the Subjects in Different Living Status that have gastritis (N=81).
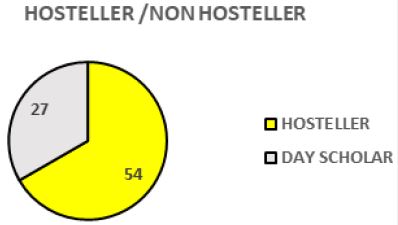
Out of 81 samples who had been diagnosed as gastritis by Doctor, there are 54 hosteller and 27 nonhostellers. Prevalence of gastritis among hosteller is higher.
Pie Chart 7 Shows Frequency of the Subjects that have Different Health Risk Behaviour that have gastritis (N=81).
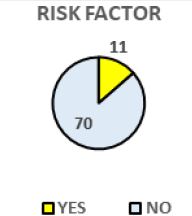
Out of 81 samples who had been diagnosed as gastritis by Doctor, 70 subjects have no specific health risk behavior, 10 of the subjects are alcoholic and 1 subject are both smoker and alcoholic among. Prevalence of gastritis among subjects who have no specific health risk behavior is higher.
Pie Chart 8 Shows Percentage of the Subjects Who had been Diagnosed as Gastritis by Doctor (N=400).
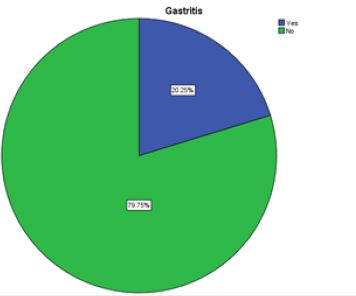
There are 20.25% subjects who had been diagnosed as Gastritis by Doctor whereas 79.75% subjects who had not been diagnosed as Gastritis by Doctor.
Discussion
Majority of the subjects with gastritis (50%) are females: This finding is same as the study conducted to
determine the correlation between students’ diet and gastritis in Faculty of Agricultural Industrial Technology
of Padjadjaran University, which showed that most of the subjects are females [1]. Most of the subjects
(83.25%) are in the age group of 21 to 23 years: This finding is similar to the finding of the study conducted
to find out the relationship among the factors influencing score and knowledge score regarding gastritis in
Sri Seshasai Educational society, which revealed that most of the subjects aged between 20-22 years [2].
An opposite observation was made to this finding of study conducted to determine the correlation between
students’ diet and gastritis in Faculty of Agricultural Industrial Technology of Padjadjaran University, which
revealed that majority of the subjects aged between 17-20 years [1]. Highest percentage of subjects (64.75%)
are Chinese. Majority of the subjects (62.50%) are MBBS students: This finding is a contradictory to the
finding of a descriptive correlative study conducted to find out the relationship between factors influencing
score and knowledge score regarding gastritis in Sri Seshasai Educational society, which revealed that most
of the subjects are post graduate students [2]. Most of the subjects (45.00%) are Year 4 students. Most of
the subjects (74.25%) are hosteller: This finding is a contradictory to the finding of a cross sectional study
conducted to find out the relationship between eating habits with the gastritis at the Medical Faculty Level
of student 2010 Sam Ratulangi University Manado, which revealed that majority of the subjects are nonhosteller
[3]. Most of the subjects (90.75%) have no specific health risk behavior: This finding is supported
by a descriptive correlative study conducted to find out the relationship between factors influencing score
and knowledge score regarding gastritis in Sri Seshasai Educational society, which revealed that majority
of the subjects have no specific health risk behavior [2]. Most of the patients (79.75%) were not diagnosed
as Gastritis by physicians. This finding is opposite to the finding of a study conducted to find out the
relationship among eating habits with the gastritis at the Medical Faculty Level of student 2010 Sam
Ratulangi University Manado, which showed that most of the subjects had gastritis [3]. Erosive gastritis
is a type of acute gastritis. Erosive gastritis is caused by the toxic damage of the mucosa of the stomach
usually due to non-steroidal anti-inflammatory drugs (NSAIDs) or drinking alcohol. Erosive gastritis may
also occur in ICU patients with sepsis, shock or major burns Endoscopy will show that these patients have
diffuse superficial erosions of the stomach mucosa and petechiae hemorrages [4]. In the olden days before
the invention of endoscopy, gastritis was a diagnosed with clinical findings and treated accordingly though
there was some degree of suspicion of malignancy of stomach. After endoscopy about 50% of the endoscopies
showed significant mucosal abnormalities. About 30% of the endoscopy revealed unexpected disease and
different modality of treatment. The advantage of doing endoscopy was less in the patients below the age of
40 years compared to older patients above 65 years with suspicion of cancer stomach or hematemesis [5].
Endoscopy picture in acute gastritis of gastric mucosa is thick, nonpliable and edematous, with erosions and
inflamed gastric folds. Endoscopy will show mucosal oedema which can be severe, causing gastric outlet
obstruction. Gastric mucosal ulcers and hemorrhagic spots. Endoscopy can also diagnose rare diseases like
gastric syphilis and tuberculosis. Endoscopy is the most important investigation of a patient with dyspeptic
symptoms to rule out malignancy. Gastroscopic examination is essential to find whether the patient’s history is organic or functional dyspepsia. Endoscopy must be done when the patient has symptoms suggestive of
gastritis and without any medical treatment, particularly antacids or PPI which will mask relevant findings
or interfere with the endoscopic findings. The major endoscopic abnormalities found are gastric ulcer (1.6-
8.2%), duodenal ulcer (2.3-12.7%), esophagitis (0-23.0%), and gastric malignancy (0-3.4%). The correlation
between the organic causes of dyspepsia and symptoms of gastritis can be different. Even after healing of the
organic cause complete symptom resolution may not occur. The correlation between the mild or equivocal
gastric mucosal inflammatory changes and dyspeptic symptoms are often confusing as there is poor or
non-existent relationship between erythematous/ exudative gastritis or duodenitis and dyspeptic symptoms
[6]. A meta-analysis has showed that the erosive esophagitis is the common disease among the individuals
who undergo endoscopy for dyspepsia., followed by peptic ulcers. Among the 240 papers evaluated, 151
showed gastritis. Erosive esophagitis was the most common disease (13.4%) followed by acid peptic disease
(8.0%). Occurrence of erosive esophagitis was less when definition of dyspepsia using Rome criteria was
used instead of common definition of gastritis (6% vs 20%). Peptic ulcer disease was common diagnosis
in individuals with gastritis than esophagitis [7]. When gastric mucosa was observed carefully the gastric
mucosal pattern under standard endoscopy can show H. pylori infection. Characteristic endoscopic findings
due to Helicobacter pylori infections are antral mucosal nodularity with thick gastric folds, and visible
prominent submucosal blood vessels. These endoscopic finding are suggesting H. pylori infection. Sometimes
the standard endoscopic features often labelled as gastritis may not be supported by gastric mucosal biopsy.
With more training, expertise, and time the magnifying endoscopy will be more diagnostic as it will show
more clearly the abnormal gastric mucosa suggesting H. pylori-infection of the stomach [8]; Recently,
high resolution magnifying endoscopy is more effective diagnostic method to diagnose gastritis. With high
resolution magnifying H. pylori gastritis is diagnosed by the specific histopathologic changes in the gastric
mucosa such as mucosal atrophy or intestinal metaplasia [9]. Gastric biopsy brings some important practical
supplement to endoscopic examination like confirming the presence of H. pylori. But it will reveal serious
pre-malignant dysplasia or malignant gastric lesions. Some study may not support it [10]. Within the past
decade the widespread use of the fiberoptic gastroscopy, gastric biopsy, and electron microscopic study of
gastric mucosa has increased our understanding of the pathophysiology of reflux gastritis. It has now been
documented by pyloric pressure measurements and gastroscopic studies that some patients with intact
stomachs may experience symptomatic reflux gastritis. Acute phlegmonous gastritis (PG) is exceedingly
rare clinical disease characterized by severe bacterial infection of the gastric wall. Early diagnosis is difficult
without endoscopy as this disease develops quickly leading on to stomach wall necrosis and peritonitis.
Acute PG carries high mortality as the diagnosis is often delayed or overlooked [11]. The magnified views
endoscopy classified H.pylori gastritis into four types based upon endoscopic finding : i) collecting venules
and true capillaries forming a network, and gastric pits which may be like pinholes (type Z-0; n = 80); ii)
irregularity of the true capillaries without collecting venules are observed (type Z-1; n = 36); iii) white
gastric pits with sulci, without collecting venules without true capillaries being seen (Z-2; n = 110); and iv)
dilated pits and surrounding redness (Z-3; n = 71). All cases without H. pylori infection - normal stomach
were type Z-0, whereas H. pylori-induced gastritis was present in all cases of Z-1, Z-2, or Z-3 classification.
The magnified endoscopy can diagnose H. pylori-related gastritis more clearly than conventional endoscopy
[12]. Magnifying narrow-band imaging (NBI) endoscopy will reveal gastric mucosal patterns and mucosal
capillary patterns. Magnifying NBI endoscopy is helpful in identifying H pylori infection early. It will
reveal the severity of gastritis histologically. It is extremely helpful in identifying gastric atrophy early. In predicting severe gastritis and gastric atrophy NBI is comparatively better than serum pepsinogen level
and regular endoscopy [13]. In a ten-year experience with 106610 diagnostics upper GI endoscopy the rate
of complications is about 0.03% and mortality rate is 2.38%. Out of 39 patients who developed endoscopyrelated
complications 5 of them underwent surgery. Out of the five patients 4 had esophageal perforations,
1 had hemorrhage following ulcer biopsy. Out of 7384 therapeutic and operative endoscopies there was no
endoscopic related mortality. In another study 44 patients developed hemorrhages after electro-excision of
the polyps [14].
Conclusion
The following conclusions are drawn based on the findings of the study: Prevalence of gastritis higher among
female, among age group 21-23 years, MBBS students, Year 4 students, hosteller is higher, respondents who
skips their breakfast, those who take hot and spicy food, who follow distracted diet.
Suggestions
After analyzing the results obtained from this study, some suggestions are given.
- Students are encouraged to avoid habit of skipping their breakfast.
- Students are encouraged to consuming less hot and spicy food and drink less coffee.
- Students are encouraged to consume enough food.
-Students are encouraged to avoid consuming citrus food on empty stomach and avoid applying distracted
diet.
Recommendations for Further Research
- Similar study must be done with more sample and at different set of people to improve the conclusive
results.
- A comparative study must be done to find out the awareness and knowledge on association of the eating
habits to the incidence of gastritis among the university students and general population.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!