Biography
Interests
Bakayoko Seydou, Sidibe Mohamed Kole*, Elien, G. Y. R. R.*, Sissoko Modibo, Diallo Seydou, Conare Ibrahima, Guindo Adama, Napo Abdoulaye, Guirou Nouhoum & Sylla, F.
Hospital and University Center of the Institute of Tropical Ophthalmology of Africa (CHU-IOTA) of the University of Sciences, Techniques and Technologies of Bamako (USTTB), Bamako, Mali
*Correspondence to: Dr. Sidibe Mohamed Kole & Elien, G. Y. R. R., Hospital and University Center of the Institute of Tropical Ophthalmology of Africa (CHU-IOTA) of the University of Sciences, Techniques and Technologies of Bamako (USTTB), Bamako, Mali.
Copyright © 2020 Dr. Sidibe Mohamed Kole & Elien, G. Y. R. R., et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
A subretinal hemorrhage (SRH) is a collection of blood located under the retina. Age-related
macular degeneration (AMD) is one of its causes, especially in the elderly.
The objective of this case report is to ask about sub-retinal hemorrhage during AMD.
This is the report of a patient managed at the IOTA-Teaching Hospital on March 14, 2020.
The patient was 83 years old, pseudophakic, known hypertensive patient, who presented with a sudden drop in visual acuity of the left eye in which the diagnosis of SRH secondary to AMD was
made.
Prognosis of the SRH can be improved by Anti VEGF intravitreal injection.
Introduction
Sub-retinal hemorrhage is an accumulation of blood under the neurosensory retina [1]. The presence of
SRH is toxic to the neurosensory retina from the twenty-fourth hour, with exacerbation of the lesions after
the seventh day of evolution [1]. There are three mechanisms for this toxicity [1,2]:
Metabolic: Sub-retinal hemorrhage forms a barrier to metabolic exchanges between the retina and the pigmentary epithelium.
Cellular: Fibrin, produced during the constitution of the hematoma, presents interdigitations between photoreceptors which, by retracting, tears off the retinal cells.
Toxic: Toxicity to retinal cells of ferrous ions from the metabolism of haemoglobin, produced by the phagocytosis of red blood cells by macrophages. This is a dose- and time-dependent phenomenon that would occur only in a second stage [1,2].
The spontaneous evolution of a sub-retinal hemorrhage leads to the profound decrease in visual acuity [1-3]. The average duration of spontaneous resorption is 5 to 8 months [1-3].
We report this case of SRH complicating AMD in this octogenarian who came to the clinic for a sudden visual acuity decrease.
Ethical Considerations
Our Paper conforms with the Declaration of Helsinki on Ethical Principles for Medical Research Involving
Human Subjects. We obtained the consent of the patient(s) for publication of this case report.
Patient Presentation
He is a pseudophakic octogenarian with a history of arterial hypertension, who came to the clinic for a
sudden drop in acuity of the left eye.
On examination we noted a visual acuity count the fingers at 1 meter on the left eye can be improved with pinhole visual acuity and the best corrected visual acuity was 4/10. The best corrected visual acuity of the right eye was 6/10. The fundus of the right eye presented serous drusens and the left eye a sub retinal macular hemorrhage with a retinal serous detachment.
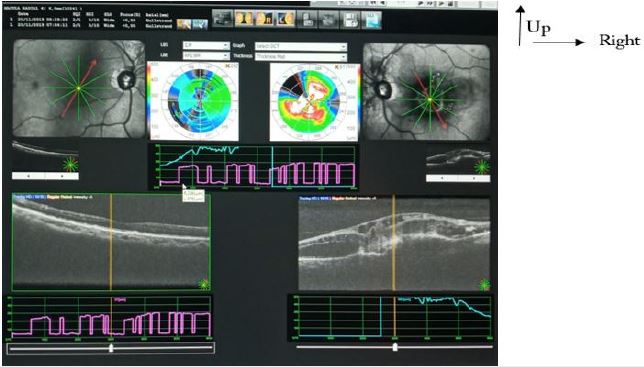
We performed optical coherence tomography, which revealed the following in the left eye: vitreofoveolar adhesion, intraretinal cysts, retinal serous detachment and haemorrhagic pigmentary epithelium and serous drusens in the contralateral eye (Fig. 1).
Management and Outcome
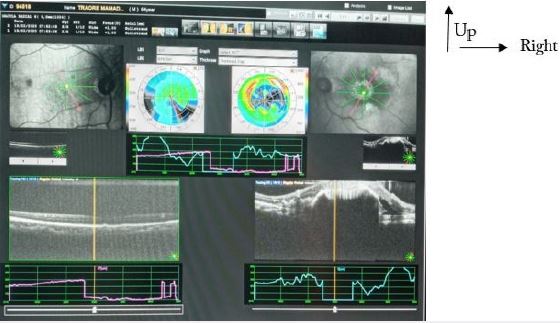
We performed 3 monthly intravitreal injections of Bevacizumab (AVASTIN®) in the left eye, followed by
a decrease in hand movement vision, a decrease in retinal serous detachment and a retrofoveolar sub-retinal
hemorrhage with a tear of the pigmentary epithelium (Figure 2).
In front of the patient’s reluctance to undergo surgical treatment, we opted for continued intravitreal injections of anti VEGF (6 injections in total) and monitoring. The visual acuity of the patient in each visit was:
1st visit: count the fingers at 1 meter 6/10
2nd visit: count the fingers at 5 meter 6/10
3rd visit: 2/10 6/10
Discussion
SRH is a rare but serious complication of AMD [2]. It has a very poor prognosis if the centre of the macula
is affected and early treatment is not given [2]. It is usually diagnosed clinically in elderly patients with a
history of vascular disease (hypertension, heart disease) or those on antiplatelet therapy and a sudden drop
in visual acuity [2,3]. Examination of the fundus may initially be difficult because of the associated presence
of vitreous hemorrhage, but more or less prominent, polycyclic lesions, retinal hemorrhages and exudates
are observed if the media are transparent [2,3]. The contribution of imaging is important for differential
diagnosis. SHR is discussed with choroidal melanoma [2-4]. From an etiopathogenic point of view, the main
pathology leading to sub-retinal hemorrhage is exudative AMD [2-4]. Exudative AMD is characterized by
the appearance of abnormal vessels (called neo-vessels) under the retina, often causing irreversible damage
to the macula. When these vessels bleed, a hematoma forms under the retina and causes damage to retinal cells [2-4]. In 2016, the CATT study analyzed the link between SRH and AMD and demonstrated the
relationship between SRH during AMD and high blood pressure [5]. Other rarer pathologies such as
retinal arterial microaneurysms, High myopia, idiopathic polypoidal choroidal vasculopathy, trauma, etc. can
also give rise to a sub-retinal hemorrhage [4,5]. The “medical” management of SRH consists of pneumatic
displacement of the hematoma by intravitreal injection of Tissue Plasminogen Activator tPA (thrombolytic
enzyme), SF6 gas and anti-VEGF [5,6]. This medical treatment is associated with paracentesis. The surgical
treatment includes a vitrectomy using gas and injection of rt-PA into the sub-retinal space [7].
Conclusion
The occurrence of a sub-retinal hemorrhage (SRH) is a dramatic complication of age-related macular
degeneration (AMD).
The current first line treatment modality is intravitreal anti-VEGF injections.
The treatment is surgical and consists of moving the hematoma by vitrectomy and injection of a tPA under the retina and gas tamponade.
Intravitreal Anti VEGF injections appear to be a safe and effective alternative in the treatment of sub-retinal hemorrhage, particularly in patients treated with aspirin or in poor general condition.
Bibliography


Hi!
We're here to answer your questions!
Send us a message via Whatsapp, and we'll reply the moment we're available!